
HER2+ Early-Stage Breast Cancer
Breast cancer is the most common malignancy in females in the U.S.1 Tumors with human epidermal growth factor receptor 2 overexpression (HER2+) constitute 15–20% of tumor subtypes and were historically associated with poor prognosis prior to the advent of HER2-targeted therapies.2,3 Neoadjuvant therapy (NAT) is preferred for most patients with early-stage HER2+ disease except those with small, node-negative tumors with the ultimate goal of obtaining pathologic complete response (pCR).4,5 A pCR, defined as no invasive disease in the breast or axillary lymph nodes, is associated with reduced risk of recurrence and improved event-free and overall survival (OS).6,7 In the event of residual disease, treatment escalation in the adjuvant setting is paramount to reduce disease recurrence and mortality.8,9
Previous Treatment Landscape
Since the FDA approval of trastuzumab, HER2-targeted therapies have transformed clinical outcomes for patients with HER2+ breast cancer.10,11 The addition of pertuzumab to trastuzumab plus chemotherapy further improved outcomes in patients with node-positive disease.12,13 These results established combining HER2-directed antibodies with chemotherapy as standard-of-care (SOC) NAT for HER2+ early-stage breast cancer (eBC).
Recent advancements in chemotherapy delivery via antibody-drug conjugates (ADCs) have ushered in a new era for treating HER2+ breast cancer. The first-generation ADC trastuzumab emtansine (T-DM1) significantly improved invasive disease-free survival (IDFS) and OS compared to adjuvant trastuzumab in patients with HER2+ eBC and residual disease following NAT in the KATHERINE trial, positioning adjuvant T-DM1 as the first SOC option for treatment escalation in patients with residual HER2+ disease.8,9 However, exploratory analyses suggested a smaller magnitude of benefit in HER2 IHC 2+/ISH+ compared to IHC 3+ tumors, as well as in those presenting with advanced locoregional disease or positive nodal status after NAT.9,14 Furthermore, adjuvant T-DM1 did not reduce central nervous system (CNS) recurrences relative to trastuzumab.14 These subgroup analyses highlight an unmet need (Table 1).
New Treatment Landscape
The next-generation ADC trastuzumab deruxtecan (T-DXd) gained a Priority Review designation indication for adjuvant therapy in patients with residual HER2+ disease at high risk for recurrence, defined as inoperable cancer (cT4, N0–3 or cT1–3, N2–3) at presentation or operable cancer (cT1–3, N0–1) with axillary node-positive disease (ypN1–3) after NAT.4
T-DXd has demonstrated robust antitumor activity across different treatment lines, including superiority relative to T-DM1 for HER2+ metastatic breast cancer (mBC).15 T-DXd has also shown CNS activity.16
The efficacy of adjuvant T-DXd was evaluated in the randomized, phase III DESTINY-Breast05 trial, which enrolled patients with high-risk HER2+ residual invasive disease. High-risk disease was defined as inoperable eBC before NAT or operable eBC with node-positive disease after NAT with a taxane plus trastuzumab ± pertuzumab.17 Patients were randomized 1:1 to receive 14 cycles of T-DXd (n=818) or T-DM1 (n=817). Stratification was based on operable status, hormone receptor status, pathological nodal status following neoadjuvant therapy, and type of HER2-targeted NAT received (i.e., single vs dual). The primary endpoint was IDFS.17 At median follow-up exceeding 29 months, most patients were <65 years old, >70% had HR+ disease, >75% received dual anti-HER2 NAT, and >80% had positive pathologic nodal status post-NAT.17 Adjuvant T-DXd led to a significant improvement in IDFS, with a 3-year rate of 92.4% compared to 83.7% with T-DM1 (HR, 0.47; 95% CI, 0.34–0.66). Most IDFS events were distant recurrences (Figure 1). CNS recurrence was numerically lower in the T-DXd arm. OS data are not yet mature. Additional results are reported in Table 1.17
Figure 1. Recurrent Disease Outcomes Associated with Adjuvant T-DXd versus T-DM1 in DESTINY-Breast05 Clinical Trial17
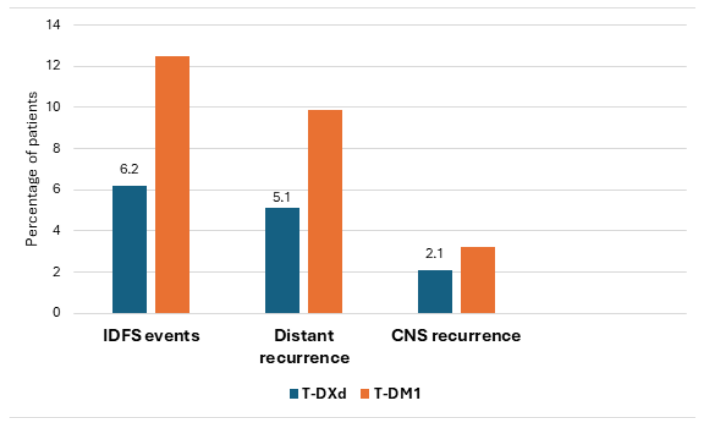
Table 1. Efficacy Results of DESTINY-Breast05 and KATHERINE Clinical Trials8,9,17,18
| DESTINY-Breast05 Clinical Trial (Adjuvant T-DXd vs T-DM1) 3-year IDFS HR (95% CI) | KATHERINE Clinical Trial (Adjuvant T-DM1 vs trastuzumab) 3-year IDFS HR (95% CI) | |
| 3-year IDFS rate, intention to treat | 92.4% vs 83.7% [HR, 0.47 (0.34-0.66)] | 88.3% vs 77% [HR, 0.5 (0.39-0.64)] |
| 3-year IDFS rate, absolute difference | 8.7% | 11.3% |
| CNS recurrence rate | 2.1% vs 3.2% | 7% vs 5.1% |
| HER2 status | IHC 3+: HR, 0.49 (0.34-0.70) IHC2+/ISH+: HR 0.35 (0.13-0.97) | IHC3+: HR, 0.47 (0.37-0.60) IHC2+/ISH+: HR 0.84 (0.56-1.25) |
| HR status | HR+ (71%): HR, 0.54 (0.35-0.82) HR – (29%): HR, 0.37 (0.22-0.65) | HR+ (71.9%): HR, 0.48 (0.35-0.67) HR – (28.1%): HR, 0.5 (0.33-0.74) |
| Disease extent at presentation (before NAT) | Operable (47.3%): HR, 0.58 (0.34-1.01) Inoperable (52.7%): HR, 0.41 (0.27-0.63) | Operable (75%): HR, 0.47 (0.33-0.66) Inoperable (25%): HR, 0.54 (0.37-0.80) |
| Pathologic LN status post NAT | ypN1-3 (80.7%): HR, 0.43 (0.29-0.62) ypN0 (19.3%): HR, 0.73 (0.33-1.59) | ypN1-3 (53.7%): HR, 0.52 (0.38-0.71) ypN0 (46.3%): HR, 0.44 (0.28-0.68) |
| NAT type | Anthracycline (51.7%): HR, 0.45 (0.29-0.69) | Anthracyclines (77.9%): HR, 0.51 (0.38-0.67) |
| HER2-targeted NAT [Single (trastuzumab) or dual (trastuzumab + pertuzumab)] | Single (21.5%): HR, 0.43 (0.22-0.84) Dual (77.9%): HR, 0.48 (0.33-0.71) | Single (80.2%): HR, 0.49 (0.37-0.65) Dual (18.7%): HR, 0.54 (0.27-1.06) |
The most common AEs with T-DXd were nausea, vomiting, and neutropenia, while thrombocytopenia and transaminitis predominated with T-DM1. Alopecia was more frequent with T-DXd (15.5% vs 1.2%). Treatment interruption and discontinuation due to AEs were higher with T-DXd. The most common reason for dose reduction was nausea with T-DXd and thrombocytopenia with T-DM1. Left ventricular (LV) dysfunction was uncommon in both arms with no grade ≥4 events (Table 2).17
Table 2. Safety Results of Adjuvant T-DXd versus T-DM1 in the DESTINY-Breast05 Clinical Trial17
| T-DXd (n=806) | T-DM1 (n=801) | |
| Completed 14 cycles | 72.3% | 76.3% |
| Most common AEs, any Grade | Nausea (71.3%), vomiting (31%), constipation (32%), neutropenia (31.6%) | Transaminitis (~50%), thrombocytopenia (49.8%) |
| Grade ≥ 3 AEs | Incidence, 50.6% (common AEs: nausea, leukopenia, neutropenia, fatigue) | Incidence, 51.9% (common AEs: thrombocytopenia, transaminitis) |
| Serious AEs | 17.4% | 13.6% |
| AEs of interest | Drug-induced ILD (9.6%, 2 Grade 5 events) Radiation pneumonitis (31.4%) | Drug-induced ILD (1.6%, no Grade 5 events) Radiation pneumonitis (30.5%) |
| LV dysfunction (any Grade, 2.9%, G1 0.1%; G2 2.5%; G3 0.2%) | LV dysfunction (any Grade, 1.7%; G1 0%; G2 1.4%; G3 0.4%) | |
| AEs leading to discontinuation | 17.9% (10.8% due to ILD) | 12.9% (2.5% due to ILD) |
| AEs leading to drug interruptions | 49.6% | 41.1% |
| AEs leading to dose reductions | 26.4% | 26.6% |
Interstitial Lung Disease (ILD) and Radiation Pneumonitis: Monitoring, Management, and Incidence in DESTINY-Breast05 Clinical Trial
Monitoring
Adjuvant radiotherapy (RT) could be administered concurrently with or prior to study treatment (sequential). ILD monitoring included baseline non-contrast low-dose (LD) chest CT, followed by LD chest CT at cycle 3 (6 weeks), then every 12 weeks (cycles 7 and 11), and at 40-day follow-up. Patients receiving sequential RT had additional LD chest CT after RT completion.
Management Guidelines
Radiation pneumonitis (RP) encompassed pulmonary radiation injury, alveolitis, bronchitis, and fibrosis. Symptomatic drug-induced ILD was defined as acute onset of new or worsening pulmonary symptoms (dyspnea, cough, fever); grade ≥2 ILD was assigned when any symptoms were present. RP attribution to radiation was determined by timing and location of radiographic abnormalities. Management guidelines are described in Table 3.17
Table 3. Drug-Induced ILD and Radiation Pneumonitis Management Guidelines per DESTINY-Breast05 Study Protocol17
| Grade 1 (asymptomatic) | Grade 2 (symptomatic) | Grades 3-4 (symptomatic) | |
| Radiation pneumonitis | Maintain dose and schedule |
|
Discontinue treatment |
| Drug-induced ILD |
|
|
|
Incidence and Severity
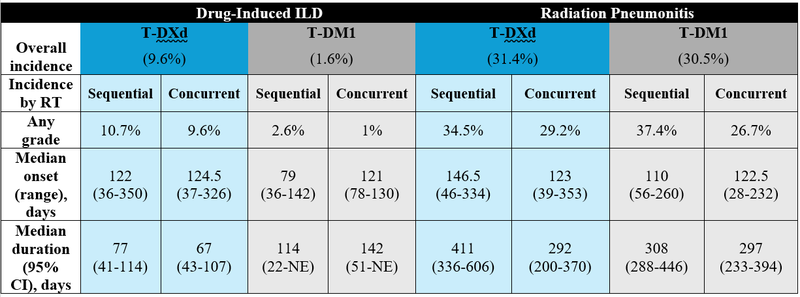
Drug-induced ILD of any grade occurred in 9.6% with T-DXd versus 1.6% with T-DM1. ILD rates in the T-DXd arm were similar with concurrent and sequential RT. By grade, ILD in the T-DXd arm was 2.1% (grade 1), 6.7% (grade 2), and 0.9% (grade 3). Grade 5 ILD occurred in two patients in the T-DXd arm. In the T-DM1 arm, no grade ≥3 ILD events occurred. RT timing did not impact ILD incidence or severity in either arm (Table 4).
All RP events were grade ≤2 in both arms. RP incidence was higher with sequential versus concurrent RT in both arms. In the T-DXd arm, sequential RT was associated with longer time to onset and duration of RP (Table 4). These findings suggest no benefit from sequencing T-DXd and RT. The differences in ILD and RP onset, duration, and outcomes between sequential and concurrent RT require further study to clarify the influence of comorbidities, race, RT practices, and steroid use. Well-designed real-world studies are needed to define risk in patients with poorer performance status, organ dysfunction, or advanced age.17,18
Table 4. Drug Induced ILD and Radiation Pneumonitis by Timing of Adjuvant Radiation18
From Clinical Trials to Practice: Adjuvant T-DXd Place in Therapy
DESTINY-Breast05 enrolled a higher-risk population than KATHERINE, with 52% versus 25% presenting with inoperable disease and 81% versus 46% with positive nodes at surgery, respectively.9,17 The trial also reflects contemporary practice, with > 75% receiving dual anti-HER2 NAT compared to <20% in KATHERINE.9,17 T-DXd demonstrated efficacy across all HER2 IHC statuses, likely due to its higher payload delivery and bystander effect, whereby the released cytotoxic payload penetrates neighboring tumor cells regardless of their HER2 expression, thus overcoming lower HER2 expression.17,18
Toxicity management is critical for treatment implementation in clinic. Treatment discontinuation occurred more frequently with T-DXd than T-DM1. Nausea, neutropenia, and alopecia were more common with T-DXd, all of which can impact quality of life when inadequately addressed.17 Increased costs may be anticipated due to recommendations for more frequent chest CT monitoring and intensive supportive care.
ILD remains the most serious AE with two fatal cases reported in a curative setting.17 Adherence to protocol-recommended chest CT monitoring is essential for detecting asymptomatic ILD early, though insurance coverage may limit feasibility.17,19 Distinguishing radiation-induced from drug-induced pneumonitis requires multidisciplinary collaboration between pulmonology and radiology.19,20 Institutions should establish relationships with pulmonology services.
Potential Changes in the Treatment Paradigm
While the DESTINY-Breast05 trial utilized T-DXd in the adjuvant setting, the DESTINY-Breast11 trial investigated T-DXd for neoadjuvant use. Sequencing questions arise with data from DESTINY-Breast11, as the appropriate treatment for patients with residual disease after neoadjuvant T-DXd remains uncertain.21 Emerging data from CompassHER2 RD (tucatinib plus T-DM1, NCT04457596) will inform treatment selection in the adjuvant setting, particularly regarding CNS recurrence risk. T-DM1 remains appropriate for patients with lower risk and smaller residual disease.9 Future directions include biomarker utilization like circulating tumor DNA clearance to guide escalating treatment for highest-risk patients, sparing lower-risk patients unnecessary toxicity and cost.
HER2+ Metastatic Breast Cancer
Many patients present with HER2+ mBC or develop metastases despite receiving neoadjuvant and adjuvant therapies for early-stage disease.22,23 HER2-amplified tumors have a predisposition to metastasize to the brain, with up to 50% of patients with HER2+ mBC developing brain metastases which is associated with the poorest prognosis.16,24
Previous Treatment Landscape
Standard first-line treatment for HER2+ mBC includes a taxane plus trastuzumab and pertuzumab (THP) for at least 6 cycles, followed by maintenance trastuzumab and pertuzumab (HP).4 Subcutaneous HP is an option and can reduce chair time in infusion centers when available.25 First line THP significantly improved both progression free survival (PFS) [HR 0.69; 95% CI, 0.59-0.81] and OS (HR 0.69; 95% CI, 0.58-0.82), establishing this regimen as SOC.4,26 In patients with HR+/HER2+ mBC, endocrine therapy (ET) ± palbociclib can be added to maintenance HP.4,27 T-DXd is the current preferred second-line treatment for HER2+ mBC based on results from the DESTINY-Breast03 trial.4,28,29
New Treatment Landscape
The phase 3 DESTINY-Breast09 trial evaluated first-line T-DXd monotherapy and T-DXd plus pertuzumab (T-DXd + P) versus THP.30 Prior treatment for HER2+ eBC was allowed if the disease-free interval was ≥6 months. Patients were randomized 1:1:1 to T-DXd + P (n=383), T-DXd + placebo (387), or THP (n=387). Patients with HR+ disease could receive ET after completing 6 cycles. The primary endpoint was PFS while key secondary endpoints included objective response rate (ORR), duration of response (DOR), and safety outcomes. Only results comparing T-DXd + P versus THP are currently available.
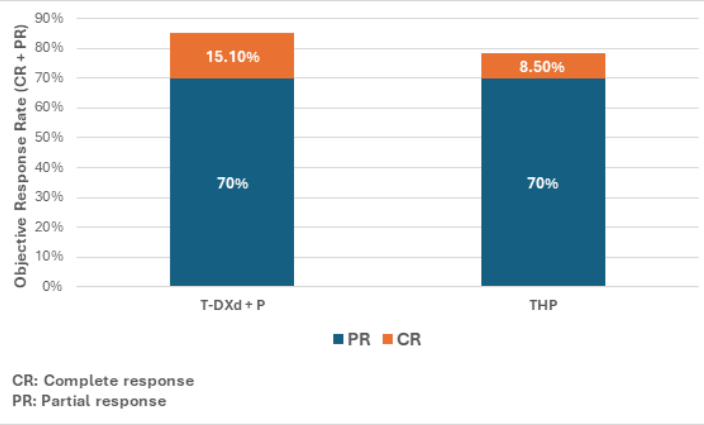
Across both groups, the median age was 54 years, >50% had de novo mBC, 28.3% received prior trastuzumab and 7.1% prior pertuzumab, <10% had CNS metastases, 54% had HR+ disease, and >30% had PIK3CA mutations. At median follow-up >29 months, median PFS was 40.7 months with T-DXd + P versus 26.9 months with THP (HR 0.56; 95% CI, 0.44-0.71).30 Benefit was observed across subgroups including HR+ disease and PIK3CA-mutated tumors. ORR was higher with T-DXd + P, with median DOR of 39.2 versus 26.4 months (Figure 2). OS data remains immature.
Figure 2. Response Rates in DESTINY-Breast09 Clinical Trial (T-DXd + P vs THP)30
Time to second progression or death (PFS2) also favored T-DXd + P (HR 0.60; 95% CI, 0.45-0.79). Notably, only 10.1% of patients in the THP arm received T-DXd and 12.1% received T-DM1 in the second-line setting.31 Grade ≥3 AEs occurred in 63.5% with T-DXd + P and 62.3% with THP. The most common AEs with T-DXd + P were nausea, vomiting, diarrhea, neutropenia, alopecia, and fatigue. Dose reductions (45.9% vs 19.9%) and interruptions (68.8% vs 49%) due to AEs occurred more frequently with T-DXd + P. Grade 5 AE incidence was higher with T-DXd + P (3.4% vs 0.8%).30 Drug-induced ILD occurred in 12.1% of patients receiving T-DXd + P (Grade 1, 4.5%; Grade 2, 7.1%; Grade 5 in 2 patients) with a median onset of 210.5 days, compared to 1% with THP (no Grade ≥3 events). LV dysfunction occurred in 11% with T-DXd + P (one Grade 4 event) versus vs 7.1% with THP.30
From Clinical Trials to Practice: T-DXd’s Place in Therapy for HER2+ Metastatic Breast Cancer
The DESTINY-Breast09 results raise important considerations for clinical implementation. Unlike THP, which allows de-escalation to maintenance HP after induction chemotherapy, T-DXd + P requires indefinite treatment until progression, increasing cumulative toxicity burden. The convenience of maintenance HP requiring no laboratory monitoring, minimal to no premedication, and freedom from gastrointestinal toxicity, neutropenia, and alopecia represents a meaningful quality-of-life advantage that must be weighed against the PFS benefit of frontline T-DXd. The phase 2 DEMETHER study (NCT06172127) is evaluating a sequential strategy of six cycles of T-DXd induction followed by maintenance with subcutaneous HP, offering a practical approach balancing efficacy with reduced long-term toxicity.
Patient selection for first-line T-DXd + P versus reserving T-DXd for second-line therapy remains nuanced. The favorable PFS2 data suggest that sequencing may matter less than ensuring patients ultimately receive T-DXd; however, only 10.1% of THP-treated patients received second-line T-DXd, limiting conclusions about optimal sequencing.31 The small proportion of patients with CNS metastases enrolled (<10%) limits applicability to this population, though T-DXd's established intracranial activity remains an important consideration when selecting first-line therapy.
Treatment selection is complicated by emerging data in HR+/HER2+ mBC. The PATINA trial demonstrated significant PFS improvement with adding palbociclib to HP plus ET in patients with at least stable disease after THP induction.27 The HER2CLIMB-05 trial showed that adding tucatinib to maintenance HP after THP induction significantly improved PFS compared to placebo with notable numerical improvement in patients with brain metastases, making tucatinib-based maintenance attractive for patients at high CNS recurrence risk.32 Results of T-DXd monotherapy from DESTINY-Breast09 are awaited to clarify whether pertuzumab adds meaningful benefit to T-DXd in the first-line setting. Given this increasing complexity of HER2-targeted sequencing and the need for vigilant toxicity monitoring, oncology pharmacists play a critical role in optimizing treatment selection, supportive care, and multidisciplinary management for patients receiving T-DXd.
References
-
Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72(6):524-541. doi:10.3322/caac.21754
-
Loibl S, Gianni L. HER2-positive breast cancer. Lancet. 2017;389(10087):2415-2429. doi:10.1016/S0140-6736(16)32417-5
-
Slamon D, Eiermann W, Robert N, et al. Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med. 2011;365(14):1273-1283. doi:10.1056/NEJMoa0910383
-
Enhertu granted Priority Review in the US as post-neoadjuvant treatment for patients with HER2-positive early breast cancer. AstraZeneca. March 9, 2026. Accessed March 21, 2026. https://www.astrazeneca.com/media-centre/press-releases/2026/enhertu-granted-priority-review-in-the-us-as-post-neoadjuvant-treatment-for-patients-with-her2-positive-early-breast-cancer.html
-
Jackisch C, Cortazar P, Geyer CE, et al. Risk-based decision-making in the treatment of HER2-positive early breast cancer: recommendations based on the current state of knowledge. Cancer Treat Rev. 2021;99:102229. doi:10.1016/j.ctrv.2021.102229
-
Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164-172. doi:10.1016/S0140-6736(13)62422-8
-
Spring LM, Fell G, Arfe A, et al. Pathologic complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: a comprehensive meta-analysis. Clin Cancer Res. 2020;26(12):2838-2848. doi:10.1158/1078-0432.CCR-19-3492
-
von Minckwitz G, Huang CS, Mano MS, et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628. doi:10.1056/NEJMoa1814017
-
Geyer CE, Untch M, Huang CS, et al. Survival with trastuzumab emtansine in residual HER2-positive breast cancer. N Engl J Med. 2025;392(3):249-257. doi:10.1056/NEJMoa2406070
-
Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353(16):1673-1684. doi:10.1056/NEJMoa052122
-
Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Trastuzumab for early-stage, HER2-positive breast cancer: a meta-analysis of 13,864 women in seven randomised trials. Lancet Oncol. 2021;22(8):1139-1150. doi:10.1016/S1470-2045(21)00288-6
-
Loibl S, Jassem J, Sonnenblick A, et al. Adjuvant pertuzumab and trastuzumab in early human epidermal growth factor receptor 2-positive breast cancer in the APHINITY trial: third interim overall survival analysis with efficacy update. J Clin Oncol. 2024;42(31):3643-3651. doi:10.1200/JCO.23.02505
-
Loibl S, Jassem J, Sonnenblick A, et al. Adjuvant pertuzumab and trastuzumab in early human epidermal growth factor receptor 2-positive breast cancer in the APHINITY trial: third interim overall survival analysis with efficacy update. J Clin Oncol. 2024;42(31):3643-3651. doi:10.1200/JCO.23.02505
-
Mamounas EP, Untch M, Mano MS, et al. Adjuvant T-DM1 versus trastuzumab in patients with residual invasive disease after neoadjuvant therapy for HER2-positive breast cancer: subgroup analyses from KATHERINE. Ann Oncol. 2021;32(8):1005-1014. doi:10.1016/j.annonc.2021.04.011
-
Hurvitz SA, Hegg R, Chung WP, et al. Trastuzumab deruxtecan versus trastuzumab emtansine in patients with HER2-positive metastatic breast cancer: updated results from DESTINY-Breast03, a randomised, open-label, phase 3 trial. Lancet. 2023;401(10371):105-117. doi:10.1016/S0140-6736(22)02420-5
-
Harbeck N, Ciruelos E, Jerusalem G, et al. Trastuzumab deruxtecan in HER2-positive advanced breast cancer with or without brain metastases: a phase 3b/4 trial. Nat Med. 2024;30:3717-3727. doi:10.1038/s41591-024-03261-7
-
Loibl S, Park YH, Shao Z, et al. Trastuzumab deruxtecan in residual HER2-positive early breast cancer. N Engl J Med. 2025. doi:10.1056/NEJMoa2514661
-
Loibl S, Park YH, Shao Z, et al. Additional efficacy and safety from the DESTINY-Breast05 study of trastuzumab deruxtecan (T-DXd) vs trastuzumab emtansine (T-DM1) in patients with high-risk human epidermal growth factor receptor 2–positive (HER2+) primary early breast cancer with residual invasive disease after neoadjuvant therapy. Presented at: San Antonio Breast Cancer Symposium; December 9-12, 2025; San Antonio, TX.
-
Wekking D, Porcu M, Pellegrino B, et al. Multidisciplinary clinical guidelines in proactive monitoring, early diagnosis, and effective management of trastuzumab deruxtecan (T-DXd)-induced interstitial lung disease (ILD) in breast cancer patients. ESMO Open. 2023;8(6):102043. doi:10.1016/j.esmoop.2023.102043
-
Cereser L, Della Rossa S, Sparascio F, et al. Chest computed tomography of trastuzumab-deruxtecan (T-DXd)-related interstitial lung disease: key points for radiologists. Eur J Radiol. 2025;194:112499. doi:10.1016/j.ejrad.2025.112499
-
Hurvitz SA, Loi S, O'Shaughnessy J, et al. Neoadjuvant trastuzumab deruxtecan vs trastuzumab and docetaxel in HER2-positive early breast cancer: DESTINY-Breast11. Lancet. 2025. doi:10.1016/S0140-6736(25)00001-5
-
Tapia M, Hernando C, Martínez MT, et al. Clinical impact of new treatment strategies for HER2-positive metastatic breast cancer patients with resistance to classical anti-HER therapies. Cancers (Basel). 2023;15(18):4522. doi:10.3390/cancers15184522
-
Tripathy D, Brufsky A, Cobleigh M, et al. De novo versus recurrent HER2-positive metastatic breast cancer: patient characteristics, treatment, and survival from the SystHERs registry. Oncologist. 2020;25(2):e214-e222. doi:10.1634/theoncologist.2019-0446
-
Kuksis M, Gao Y, Tran W, et al. The incidence of brain metastases among patients with metastatic breast cancer: a systematic review and meta-analysis. Neuro Oncol. 2021;23(6):894-904. doi:10.1093/neuonc/noaa285
-
Genentech, Inc. Phesgo (pertuzumab, trastuzumab, and hyaluronidase-zzxf) injection prescribing information. South San Francisco, CA; 2024
-
Swain SM, Miles D, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2020;21(4):519-530. doi:10.1016/S1470-2045(19)30863-0
-
Metzger O, Mandrekar S, Goel S, et al. Palbociclib for hormone-receptor-positive, HER2-positive advanced breast cancer. N Engl J Med. 2026;394(5):451-462. doi:10.1056/NEJMoa2511218
-
Cortés J, Kim SB, Chung WP, et al. Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. N Engl J Med. 2022;386(12):1143-1154. doi:10.1056/NEJMoa2115022
-
Cortés J, Hurvitz SA, Im SA, et al. Trastuzumab deruxtecan versus trastuzumab emtansine in HER2-positive metastatic breast cancer: long-term survival analysis of the DESTINY-Breast03 trial. Nat Med. 2024;30(8):2208-2215. doi:10.1038/s41591-024-03060-0
-
Tolaney SM, Jiang Z, Zhang Q, Barroso-Sousa R, Park YH, Rimawi MF, Saura C, Schneeweiss A, Toi M, Chae YS, Kemal Y, Chaudhari M, Şendur MAN, Yamashita T, Casalnuovo M, Danso MA, Liu J, Shetty J, Herbolsheimer P, Loibl S; DESTINY-Breast09 Trial Investigators. Trastuzumab Deruxtecan plus Pertuzumab for HER2-Positive Metastatic Breast Cancer. N Engl J Med. 2025 Oct 29. doi: 10.1056/NEJMoa2508668
-
Tolaney SM, Jiang Z, Zhang Q, et al. Trastuzumab deruxtecan plus pertuzumab for HER2-positive metastatic breast cancer. N Engl J Med 2026;394:551-62. DOI: 10.1056/NEJMoa2508668. Supplementary appendix
-
Dieras V, Curigliano G, Martin M, et al. HER2CLIMB-05: A Phase III Study of Tucatinib Versus Placebo in Combination With Trastuzumab and Pertuzumab as First-Line Maintenance Therapy for HER2+ Metastatic Breast Cancer. J Clin Oncol. 2025 Dec 10:JCO2502600. doi: 10.1200/JCO-25-02600


