Introduction
Cancer is diagnosed in approximately 1 in 1,000–2,000 pregnancies, a frequency that has increased alongside delayed childbearing and rising cancer incidence in younger adults.1 Pregnancy-associated malignancies largely mirror those seen in reproductive-age women, with breast and cervical cancers accounting for nearly half of cases, followed by hematologic malignancies and melanoma.2 Physiologic changes of pregnancy may obscure early oncologic symptoms, contributing to diagnostic delay and more advanced-stage presentation compared with nonpregnant patients.3
Management is uniquely complex. Randomized clinical trials in pregnant populations are neither feasible nor ethical, leaving clinicians to rely on observational data, registries, and pharmacologic principles. Simultaneously, gestational physiology alters drug pharmacokinetics and placental transfer, requiring careful interpretation of safety data while generally maintaining standard weight-based chemotherapy dosing.4-10
Dual diagnoses place intense emotional and ethical demands on patients and clinicians. Structured, evidence‑informed guidance is essential. The 2025 American Society of Clinical Oncology (ASCO) management of cancer during pregnancy guideline synthesizes available data to support balanced, multidisciplinary decision-making that prioritizes maternal oncologic outcomes while thoughtfully addressing fetal risk. This review highlights key updates from the guideline and discusses their practical implications on multidisciplinary cancer care, including that provided by oncology pharmacists.
Scope and Methodology of the ASCO Guideline
Unlike many ASCO guidelines, this guidance leans heavily on multidisciplinary expertise rather than randomized controlled trials. In this setting, structured, deliberative, and multidisciplinary clinical judgment plays a central role in translating limited evidence into practical guidance.
The guideline addresses three overarching clinical questions: 1. Diagnostic evaluation of suspected malignancy during pregnancy; 2. Oncologic management of newly diagnosed or recurrent cancer; 3. Obstetrical management considerations beyond routine prenatal care. A multidisciplinary Expert Panel conducted a systematic literature review. The group included oncologists, maternal-fetal medicine specialists, obstetricians, radiologists, neonatologists, pharmacists, ethicists, and methodologists. After eligibility screening, 450 studies informed the final recommendations. Evidence quality was appraised using risk-of-bias tools and GRADE methodology; however, in areas where high-level data were unavailable, consensus and expert interpretation were required. Draft recommendations underwent public comment, external review, and ASCO Evidence-Based Medicine Committee approval prior to publication.
General Principles: Prioritize Maternal Survival, Individualize by Trimester
This ASCO guidance emphasizes a foundational principle: optimal maternal outcomes are the strongest determinant of fetal outcomes. In pregnancies complicated by cancer, particularly prior to fetal viability, preservation of maternal health must remain the primary therapeutic objective. Pharmacists should recognize that systemic therapy decisions are therefore framed first by oncologic urgency and expected maternal benefit, with fetal risk contextualized within that framework. Transparent counseling is essential and should include discussion of anticipated maternal outcomes, potential fetal risks, reasonable therapeutic alternatives, and the option of pregnancy termination (where legally permissible and clinically appropriate).11,12
Informed consent in this setting is multidisciplinary and longitudinal rather than episodic. It should explicitly address the risks of treatment initiation, modification, or delay, including the oncologic consequences of postponement. Pharmacists play a critical role in these discussions by clarifying drug-specific teratogenicity data, placental transfer characteristics, timing considerations, and supportive care implications.
Gestational age substantially influences therapeutic options. First-trimester exposure to cytotoxic chemotherapy is associated with the highest risk of structural malformations due to organogenesis and is generally avoided when possible. In contrast, the second and third trimesters allow for broader use of surgery and selected systemic therapies, as the risk profile shifts from teratogenesis toward growth restriction, preterm birth, and myelosuppression. Pharmacists should ensure regimen selection and supportive care plans reflect these trimester-specific risk profiles.
Structured multidisciplinary collaboration improves both decision quality and documentation integrity. Dedicated tumor board processes that include medical oncology, maternal–fetal medicine, neonatology, radiology, pharmacy, social work, and ethics support consistent application of evidence-based recommendations and mitigate variability in care. Within this structure, pharmacists contribute expertise in pharmacokinetics during pregnancy, dose modification considerations, timing of therapy relative to delivery, and neonatal exposure risk, ensuring alignment with ASCO’s emphasis on coordinated, patient-centered care.11
Systemic Therapy During Pregnancy: What’s New and What’s Settled
Therapy During Pregnancy: Practical Guidance for Oncology Pharmacists
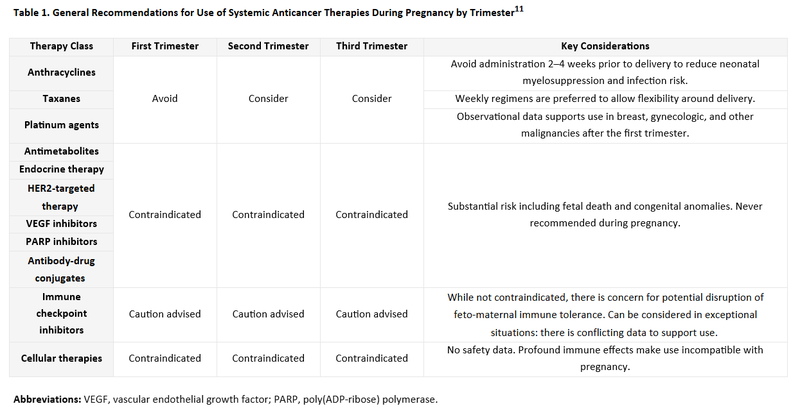
For oncology pharmacists, the most important takeaway from the ASCO guidance is that treatment during pregnancy is neither experimental nor improvised. In many cases, there is a well-established framework to guide safe and effective therapy.11,12 The role of the pharmacist is to apply that framework thoughtfully, anticipate timing and toxicity issues, and support clear counseling. Table 1 provides class-specific trimester considerations, and the discussion below highlights how to operationalize those principles in practice.
Chemotherapy (Primarily Second and Third Trimester)
Cytotoxic chemotherapy in the second and third trimesters is now a settled area of practice for several common regimens. ASCO affirms that anthracyclines, taxanes, and platinum agents can be administered during these trimesters when maternal benefit warrants treatment. The key implementation principles are straightforward include avoiding first-trimester exposure, when possible, due to fetal organogenesis and avoiding chemotherapy administration within approximately two to four weeks of anticipated delivery to reduce the risk of neonatal cytopenias.11
Oncology pharmacists should focus on aiding the oncology team coordinate timing of treatment. Typically, in these cases, the medical oncologist works in close collaboration with the maternal fetal medicine provider. In coordination with the medical oncologist, the due date should be closely tracked to confirm gestational age as well as clearly clarify anticipated delivery planning. For example, if a patient needs to deliver via C-section at 35 weeks with twins per guidance from the MFM, then the oncology team should help coordinate chemotherapy around this event. In breast and cervical cancer, observational cohorts and systematic reviews consistently demonstrate favorable short-term neonatal outcomes and acceptable maternal disease control when regimens are selected appropriately.16-18 Premature delivery is common but is often planned rather than spontaneous so that treatment can be adequately planned around delivery. When counseling, it is reasonable to communicate that while long-term pediatric data are limited, available follow-up is generally reassuring.11,16,17 The tone when counseling patients should reflect cautious confidence rather than alarm.
Targeted Therapy
Although targeted therapies remain largely contraindicated during pregnancy, they require more individualized assessment.11,21 Unlike cytotoxic chemotherapy, safety cannot be inferred from drug class alone. Decisions hinge on available human and animal model data, known or suspected fetal toxicity, degree of placental transfer, maternal complications, and whether risk is trimester-dependent or absolute.11 See Table 1 for guidance on specific agents.
Immune Checkpoint Inhibitors
Immune checkpoint inhibitors (ICI) are an area of growing evidence and thus warrant more advanced counseling. As a general rule, ASCO advises against ICIs during pregnancy due to the theoretical potential for disruption of fetomaternal immune tolerance and IgG placental transfer in late gestation.11 Case series reported prematurity and complications of pregnancy, and postpartum initiation is preferred where possible.19
ASCO appropriately frames decisions to use ICIs within multidisciplinary review and ethics‑informed consent.11 For pharmacists, the priority is balanced communication: acknowledge the uncertainty, explain the mechanism‑based concerns, and support shared decision‑making without overstating either risk or reassurance.11,19,20
Other Therapies
Some therapies remain unequivocally contraindicated. Endocrine agents such as tamoxifen and aromatase inhibitors, as well as methotrexate, should not be used during pregnancy because of established teratogenicity. These recommendations are stable and clear.
Chimeric antigen receptor (CAR) T‑cell therapy is contraindicated during pregnancy. There are no human or animal data evaluating its safety in this setting. Given the potential for transplacental passage of genetically modified immune cells, fetal toxicity cannot be excluded.11
Interferon‑alpha's large molecular weight limits placental transfer, and it has not been associated with fetal malformations, making it relatively safe throughout pregnancy.11,22,23
Local Therapies: Surgery and Radiation
For oncology pharmacists, local therapy decisions intersect with systemic sequencing, perioperative medication management, and coordination of adjuvant treatment in alignment with delivery planning.
Surgery remains a cornerstone of cancer management during pregnancy and can be performed safely during any trimester when coordinated by experienced multidisciplinary teams. Maternal and fetal risks are mitigated through careful consideration of gestational age, surgical urgency, operative approach, and anesthetic planning. ASCO highlights site‑specific considerations across tumor types including breast, gynecologic, thyroid, gastric, renal cancers, and melanoma.
Radiation therapy, in contrast, is generally avoided during pregnancy because of fetal radiation exposure, with the highest risk occurring in the first trimester. Abdominal and pelvic radiation is contraindicated throughout pregnancy. When radiation is essential for disease control and cannot be deferred, the radiation oncology team should maintain cumulative fetal exposure below 100 mGy, utilize fetal shielding strategies, and avoid abdominal or pelvic fields.11
Neonatal Care and Lactation
Neonatal teams should be engaged early for fetal growth surveillance and postnatal monitoring, particularly after in‑utero chemotherapy exposure.11 Regarding breastfeeding, ASCO provides drug‑specific guidance post‑partum. Lactation is contraindicated during active systemic therapy. However emerging data suggest breastfeeding following breast cancer treatment completion is safe and does not increase recurrence, including in BRCA carriers which is useful for survivorship counseling once therapy is complete.11,24
Ethical, Psychosocial, and Health Equity Considerations
ASCO foregrounds autonomy and shared decision‑making, including explicit counseling that pregnancy termination may be medically necessary in emergencies to prevent death or major morbidity, or to enable optimal cancer therapy which is subject to laws and institutional policy. In complex cases, ethics consultation and, when relevant, legal counsel are recommended.1,26
The document also highlights the psychosocial weight of dual diagnoses and urges systematic referral to mental health and social resources, while recognizing disparities in access to high‑risk obstetrics specialized in oncology. Data dissemination via ASCO is intended to narrow care gaps across settings.12
Knowledge Gaps and Research Priorities
The evidence guiding cancer treatment during pregnancy remains limited. Most data are derived from animal studies, retrospective analyses, and registry reports rather than randomized trials, leaving important questions about long‑term maternal and child outcomes.
There is also heterogeneity between tumor types, drug regimens, and gestational period, making the interpretation more puzzling. Positive outcomes are more likely to be reported, and negative or missing follow‑up data may not be documented as frequently. Such limitations highlight the need for specific, interdisciplinary recommendations to be made, based on a well-founded risk–benefit framework.11
Continuing prospective registries such as international collaboration (e.g., in INCIP or the Cancer and Pregnancy Registry) are needed to enhance the level of evidence.27,28 Increased enrollment and a longer-term follow-up time frame will more accurately capture developmental effects as well as rare toxicities.29,30 More pharmacokinetic studies are needed to better understand the effects of pregnancy‑related physiologic states on the metabolism and transfer of the antineoplastic drugs.11
Conclusion
Pregnancy events overlapping with cancer diagnoses require coordinated, multidisciplinary care by prioritizing maternal survival and consideration of fetal risk within that framework. The 2025 ASCO guideline states that pregnancy should not automatically mean that anticancer regimens cannot be used. Many standard treatments can proceed safely if timing, regimen selection, and delivery planning are in sync. Pharmacists in oncology interpret emerging safety data, improve supportive management, and support evidence-based and shared decision-making. With the development of more registries and pharmaceutical knowledge, more reliable evidence will be available which will lead to better-targeted, person-oriented care.
References
-
Schwab R, Anic K, Hasenburg A. Cancer and pregnancy: a comprehensive review. Cancers (Basel). 2021;13:3048.
-
Galati F, Magri V, Arias-Cadena PA, et al. Pregnancy-associated breast cancer: a diagnostic and therapeutic challenge. Diagnostics (Basel). 2023;13:604.
-
de Haan J, Lok CAR, Schutte JS, et al. Cancer-related maternal mortality and delay in diagnosis and treatment: a case series of 26 cases. BMC Pregnancy Childbirth. 2018;18:10.
-
Benoit L, Mir O, Vialard F, et al. Cancer during pregnancy: a review of preclinical and clinical transplacental transfer of anticancer agents. Cancers (Basel). 2021;13:1238.
-
Triarico S, Rivetti S, Capozza MA, et al. Transplacental passage and fetal effects of antineoplastic treatment during pregnancy. Cancers (Basel). 2022;14:3103.
-
Roesch E, Maggiotto A, Valente SA. Multidisciplinary management of pregnancy-associated breast cancer. JCO Oncol Pract. 2025;21:313-321.
-
Loibl S, Azim HA Jr, Bachelot T, et al. ESMO expert consensus statements on the management of breast cancer during pregnancy (PrBC). Ann Oncol. 2023;34:849-866.
-
Amant F, Berveiller P, Boere IA, et al. Gynecologic cancers in pregnancy: guidelines based on a third international consensus meeting. Ann Oncol. 2019;30:1601-1612.
-
Wolters V, Heimovaara J, Maggen C, et al. Management of pregnancy in women with cancer. Int J Gynecol Cancer. 2021;31:314-322.
-
Hepner A, Negrini D, Hase EA, et al. Cancer during pregnancy: the oncologist overview. World J Oncol. 2019;10:28-34.
-
Loren AW, Lacchetti C, Amant F, et al. Management of cancer during pregnancy: ASCO guideline. J Clin Oncol. 2025;44(3):200‑251. doi:10.1200/JCO-25-02115.
-
The ASCO Post. New ASCO Guideline Addresses Management of Cancer During Pregnancy, From Diagnosis Through Survivorship. January 25, 2026.
-
American College of Obstetricians and Gynecologists. Committee opinion no. 723: Guidelines for Diagnostic Imaging During Pregnancy and Lactation. October 2017 (interim update).
-
American College of Radiology. ACR Manual on Contrast Media. 2025 ed.
-
Bookwalter CA, McDonald RJ, Packard AT, et al. Contrast media in pregnant and lactating patients, from the AJR special series on contrast media. AJR Am J Roentgenol. 2024;224(4). doi:10.2214/AJR.24.31415.
-
Wang M, Yin Z, Miao J, Wu Y. The fetal outcomes after neoadjuvant platinum and paclitaxel chemotherapy during pregnancy: analysis of three cases and review of the literature. Arch Gynecol Obstet. 2022;305:49‑54.
-
Bernardini F, Ferrandina G, Ricci C, et al. Neoadjuvant chemotherapy in pregnant patients with cervical cancer: a monocentric retrospective study. Curr Oncol. 2022;29(8):5702‑5714.
-
Song Y, Liu Y, Lin M, Sheng B, Zhu X. Efficacy of neoadjuvant platinum‑based chemotherapy during the second and third trimester of pregnancy in women with cervical cancer: an updated systematic review and meta‑analysis. Drug Des Devel Ther. 2018;13:79‑102.
-
Andrikopoulou A, Korakiti AM, Apostolidou K, Dimopoulos MA, Zagouri F. Immune checkpoint inhibitor administration during pregnancy: a case series. ESMO Open. 2021;6(5):100262.
-
Gougis P, Hamy A‑S, Jochum F, et al. Immune checkpoint inhibitor use during pregnancy and outcomes in pregnant individuals and newborns. JAMA Netw Open. 2024;7(4):e245625. doi:10.1001/jamanetworkopen.2024.5625.
-
Loibl S, Azim HA Jr, Bachelot T, et al. ESMO expert consensus statements on the management of breast cancer during pregnancy (PrBC). Ann Oncol. 2023;34(10):849‑866.
-
Zhang M, Fu S, Ren D, et al. Maternal and fetal outcomes after interferon exposure during pregnancy: a systematic review with meta‑analysis. Front Reprod Health. 2021;3:702929.
-
Schrickel L, Heidel FH, Sadjadian P, et al. Interferon‑alpha for essential thrombocythemia during 34 high‑risk pregnancies: outcome and safety. J Cancer Res Clin Oncol. 2021;147:1481‑1491.
-
The ASCO Post. Two recent studies provide evidence that breastfeeding after breast cancer may be safe. September 16, 2024.
-
ecancer. ESMO 2024: Breastfeeding after breast cancer is safe. September 14, 2024.
-
Guideline Central. Management of cancer during pregnancy — ASCO guideline summary. Published December 11, 2025; updated February 17, 2026.
-
de Haan J, Verheecke M, Van Calsteren K, et al. Oncological management and obstetric and neonatal outcomes for women diagnosed with cancer during pregnancy: a 20‑year international cohort study of 1170 patients (INCIP). Lancet Oncol. 2018;19(3):337‑346.
-
ClinicalTrials.gov. Maternal cancer diagnosis and treatment during pregnancy: a database for maternal, fetal, and neonatal outcomes (NCT02749474). Updated June 10, 2024.
-
Huis in ’t Veld EA, Van Assche IA, Van Calsteren K, et al. Long‑term development of 12‑ and 15‑year‑old offspring after maternal cancer diagnosis during pregnancy: a prospective multicentre cohort study. Ann Oncol. 2025;36(9):1025‑1034.
-
Maggen C, Wolters VERA, Cardonick E, et al. Pregnancy and cancer: the INCIP Project. Curr Oncol Rep. 2020;22:17.