
Introduction
Since the first immune checkpoint inhibitor (ICI) was approved over a decade ago, there has been significant growth in the number of available agents, with widespread expansion across various solid tumor types. With initial drug approval typically in the setting of advanced or metastatic disease, the treatment paradigm has shifted in recent years, with continual movement to earlier stages. KEYNOTE-522, published in 2020, was the first randomized phase III trial to show benefit with the addition of an ICI to systemic chemotherapy in the perioperative setting. Subsequently, this led to the first perioperative ICI approval in a solid tumor and changed standard treatment for early-stage triple-negative breast cancer (TNBC).1 Since then, a multitude of ICIs now have data supporting their use in either the neoadjuvant or adjuvant settings, or both before and after surgery as part of perioperative regimens. Simultaneously, targeted therapy for actionable genomic alterations (AGAs) in non-small cell lung cancer (NSCLC) has also expanded, oftentimes with several targeted options available for a specific biomarker in the advanced or metastatic setting.2 Like the trajectory of ICIs, recent data has evaluated the impact of targeted therapy in the setting of resectable NSCLC.3,4 This article aims to review the general shift of ICIs and targeted therapy from the advanced/metastatic to the neoadjuvant and perioperative settings across solid tumors, the rationale for administration earlier in the course of disease, use of surrogate endpoints, and clinical implications for oncology pharmacists.
Rationale for Neoadjuvant or Perioperative Use of Immune Checkpoint Inhibitors
The benefits of administering systemic therapy in the neoadjuvant setting are well established and include increased likelihood of surgical resectability via tumor downstaging, elimination of micrometastases, and early assessment of response to therapy.5,6 Indeed, achievement of a pathological complete response (pCR) following neoadjuvant chemotherapy has been associated with improved long-term outcomes in many tumor types.7,8 The recent addition of ICIs to neoadjuvant chemotherapy aims to build upon these traditional goals by utilizing the existing tumor antigens to boost systemic anti-tumor immunity and improve patient outcomes.5 Administering ICIs in this setting, while the primary tumor and any associated lymph nodes remain intact, capitalizes on the use of existing tumor-specific T-cells to generate a more expansive and robust T-cell response.6,9 This is in contrast to adjuvant ICIs administered following surgical resection, which may limit the neoantigen burden, possibly resulting in reduced T-cell activation and expansion.6 After resection of the primary tumor, these activated and now more diverse T-cells continue their work against micrometastases that could subsequently lead to relapse in the post-surgical setting.6,9 Finally, combining ICIs with cytotoxic chemotherapy may create a synergistic effect.10 Once tumor cells are killed by chemotherapy, this leads to a better T-cell/cancer cell ratio with an increased release of antigens for the immune system to target within the tumor microenvironment.10
Several trials have changed the treatment paradigm across a variety of solid tumors, moving ICIs to the perioperative space. Most of these trials employed surrogate markers including pathologic complete response (pCR) and/or event-free survival (EFS) as the primary endpoint(s), with overall survival (OS) often a key secondary outcome. It is anticipated that this treatment approach will continue to expand, with phase II trials of perioperative ICI-based regimens ongoing in additional malignancies including hepatocellular carcinoma (PRIMER-1/NCT05185739)11 and renal cell carcinoma (NCT04393350)12, for example. Table 1 highlights select randomized phase III trials that have evaluated ICIs in the perioperative setting.
Perioperative Targeted Therapy for NSCLC
Most perioperative trials evaluating the addition of ICIs either excluded patients with EGFR mutations or included such small numbers as to preclude any determination of a benefit in this population.13,14 Noting the benefits observed in the ADAURA trial evaluating adjuvant osimertinib, the phase III neoADAURA trial sought to investigate the impact of neoadjuvant osimertinib on major pathologic response (MPR) in patients with stage II-IIIB EGFR-mutated NSCLC.3,15 MPR was defined as 10% or less residual primary tumor at the time of an R0 resection. The study found that neoadjuvant osimertinib with or without chemotherapy significantly improved the rates of MPR compared to chemotherapy alone. Of note, approximately 80% of patients were able to continue osimertinib in the adjuvant setting. Data was immature for the secondary endpoint of EFS; however, in an exploratory analysis, all but one EFS event at the time of data cut-off occurred in patients who did not achieve an MPR.3
In patients with potentially resectable ALK-positive NSCLC, the phase II ALNEO trial assessing perioperative alectinib met its primary endpoint, with 46% achieving an MPR.4 Trials evaluating neoadjuvant and perioperative targeted therapy in NSCLC are ongoing. For example, the phase II NAUTIKA1 umbrella trial (NCT04302025) is evaluating various targeted therapies in the neoadjuvant and adjuvant settings for early NSCLC with AGAs.16 Though data surrounding perioperative targeted therapy in NSCLC continues to evolve, it underscores the importance of molecular testing prior to therapy selection.
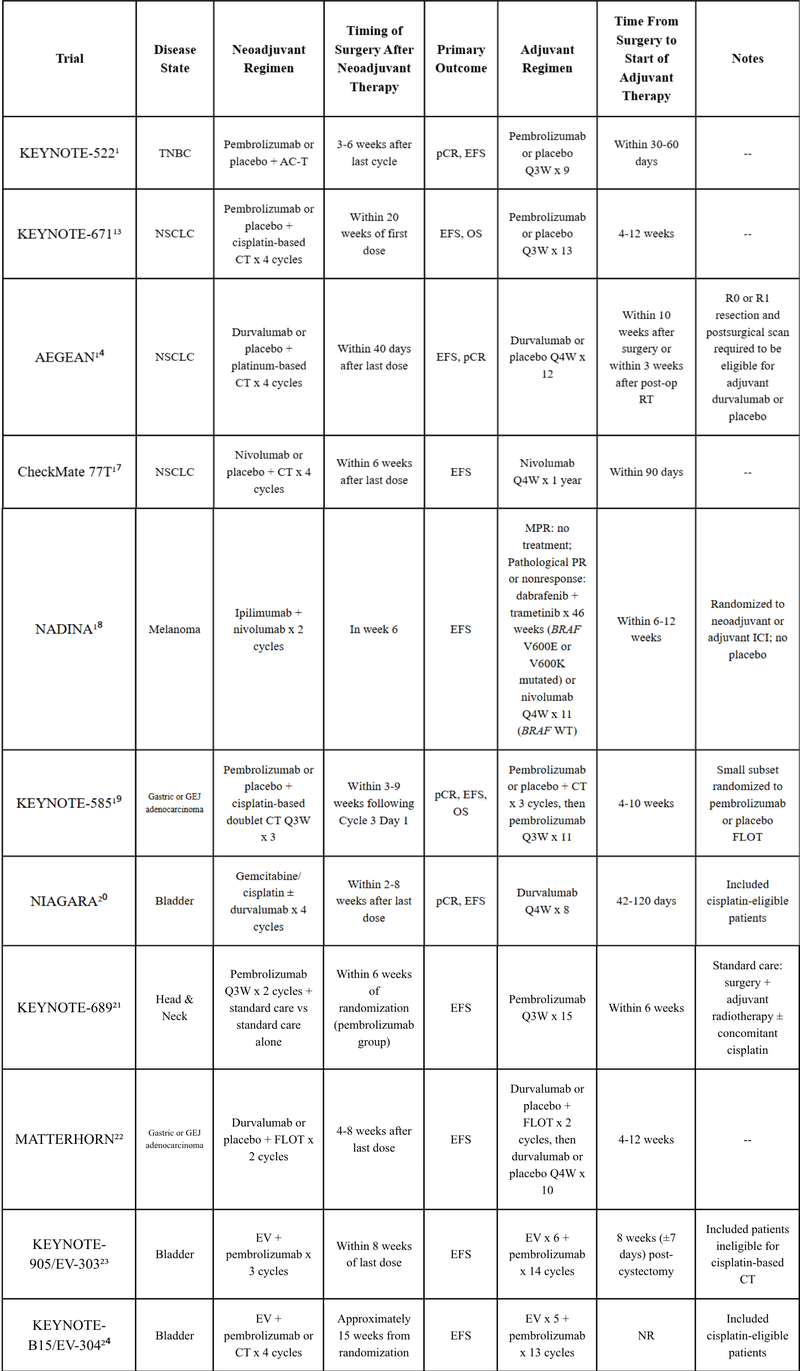
*List of trials not all inclusive and may not reflect current FDA approvals and/or guideline recommendations.
CT = chemotherapy; EV = enfortumab vedotin; GEJ = gastroesophageal junction; MPR = major pathological response; NR = not reported; PR = partial response; RT = radiotherapy; WT = wild type
Growing Role of Surrogate Pathologic Endpoints
Historically, the objective response rate based on radiologic assessment using Response Evaluation Criteria in Solid Tumors (RECIST) has been the most common surrogate endpoint for the FDA’s Accelerated Approval Program.25 However, perioperative ICI trials have shown that radiologic assessment of response after neoadjuvant treatment and before surgery routinely underestimates the treatment effect. At the time of surgery, pathologic assessment has illustrated that the tumor bed is frequently overtaken by stromal or fibrous tissue, which may incorrectly appear as an increase in or no change in tumor size on imaging despite elimination of cancer cells.10 While this phenomenon precludes the use of RECIST for assessing outcomes in neoadjuvant ICI trials, there is a unique opportunity for pathologic review, given the ability to obtain tissue both before and after ICI-based therapy, which is not routinely possible in the setting of advanced or unresectable tumors.5
Pathological response (PR) as a measure to indicate response to neoadjuvant therapy is obtained relatively quickly compared to long-term survival outcomes. However, unlike RECIST, the definition of PR in neoadjuvant ICI clinical trials has not been coordinated across solid tumor types.6 For example, the KEYNOTE-522 trial in TNBC assessed for pCR as a co-primary endpoint, defined as no invasive cancer in the breast and negative nodes according to definitions of the pathological stages ypT0/Tis ypN0, ypT0 ypN0, and ypT0/Tis.1 In NSCLC, the AEGEAN trial similarly assessed pCR as a co-primary endpoint, yet defined it as the absence of any viable tumor cells after complete evaluation of the resected tumor and sampled lymph nodes, with an MPR defined as 10% or less of viable tumor cells in the primary tumor.14 The NADINA trial included PR as a secondary endpoint according to the International Neoadjuvant Melanoma Consortium (INMC) criteria, for which PRs are expressed based on the percentage of viable tumor remaining, including pCR (0%), pathological near-complete response (10% or less), pathological partial response (11-50%), and pathological non-response (greater than 50%).18
While perioperative therapy continues to evolve, the relationship between PR and the impact of ICI and targeted therapy on survival outcomes in this setting continues to be elucidated. Prior to the introduction of perioperative ICIs, data supported an association between PR and survival for patients receiving neoadjuvant chemotherapy or chemoradiotherapy.26-28 Current evidence from some neoadjuvant ICI trials suggests PR is a prognostic marker for EFS, particularly in TNBC, NSCLC, and melanoma.6 For example, the AEGEAN trial reported a significantly improved 24-month EFS rate of 63.3% in the durvalumab group compared with 52.4% receiving placebo, with 17.2% vs 4.3% achieving a pCR, respectively.14 However, pCR does not consistently correlate with improved survival. Although KEYNOTE-585 found a better pCR rate in the pembrolizumab arm (13.4% vs 2.0%), median EFS (44.4 vs 25.7 months) and OS (71.8 vs 55.7 months) did not meet the prespecified threshold for significance in the main cohort.29 Correlating PR with long-term outcomes likely would allow for shorter turnaround time from clinical trial data reporting to FDA approvals, as EFS or OS is typically favored over PR for these decisions.10 For example, while the KEYNOTE-522 trial data were initially published in February 2020, the FDA approved perioperative pembrolizumab for early-stage TNBC in July 2021 once the co-primary endpoint of EFS was met.1,30
While it remains unclear if pCR is a true surrogate marker across all solid tumor types, efforts are ongoing to standardize PR criteria. In November 2025, the Society for Immunotherapy of Cancer and INMC published an updated pan-tumor guideline for neoadjuvant scoring of PR.31 With this, PR is measured by assessing the percentage of residual viable tumor (%RVT), determined by the proportion of viable tumor after neoadjuvant therapy in relation to the tumor before therapy, as well as the percentage of regression and necrosis. It is recommended that these percentages be reported at 10% intervals, or if between 1% and 5%, as single percentages. This continuum of PRs, ranging from 0-100%, will allow standardization across solid tumor types and may allow for inverse correlation with improved patient outcomes. For example, PR from an analysis of the phase III CheckMate 816 trial evaluating neoadjuvant nivolumab plus chemotherapy in resectable NSCLC concluded that each 1% increase in RVT was associated with a 0.017 increase in the hazard ratio for EFS.3
Clinical Considerations for Oncology Pharmacists
As the landscape of perioperative ICIs continues to evolve, oncology pharmacists maintain their crucial role on the multidisciplinary healthcare team by staying informed of new data and developments to treatment paradigms, advising on logistics of therapies, providing education, and assisting with toxicity monitoring. Currently, most reported trials have administered adjuvant ICI-based therapy regardless of response. Notably, the NADINA trial utilized a response-adapted approach.18 Questions remain as to how much adjuvant ICIs contribute to the overall benefit in those with a pCR or MPR and the optimal duration of adjuvant ICIs.33 For example, in the CheckMate 816 trial evaluating neoadjuvant chemoimmunotherapy in NSCLC, recurrence rates were low in those who achieved a pCR.33,34 Recurrence rates were also low in the NADINA trial in melanoma, where patients with an MPR did not receive an adjuvant ICI.18 Future studies will hopefully aid in defining more individualized adjuvant treatment decisions via a risk- or response-adapted approach.
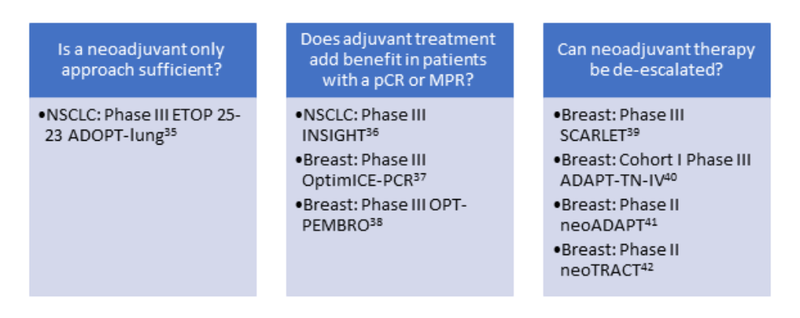
Figure 1 provides examples of ongoing trials that aim to answer remaining clinical questions regarding the optimal approach to neoadjuvant and perioperative ICIs.33 In NSCLC, the goal of the ETOP 25-23 ADOPT-lung study (NCT06284317) is to determine whether a neoadjuvant-only approach is sufficient by evaluating the impact of the adjuvant portion of perioperative chemoimmunotherapy in patients with resected stage IIB-IIIB (N2) NSCLC.33,35 Following 3-4 cycles of neoadjuvant durvalumab plus platinum-based chemotherapy and surgery, patients with a complete resection (R0 and R1) will be randomized to either adjuvant durvalumab or observation. The primary outcome is DFS in patients who did not achieve a pCR.35
The INSIGHT trial (NCT06498635) will compare DFS among patients with stage II-IIIB NSCLC who achieved a pCR following neoadjuvant chemoimmunotherapy, randomizing to adjuvant durvalumab or surveillance.36 In early-stage TNBC, the goals of the OptimICE-PCR (NCT05812807) and OPT-PEMBRO trials (NCT06606730) are to determine the benefit of adjuvant pembrolizumab in patients who have achieved a pCR following completion of neoadjuvant chemoimmunotherapy.37,38 Additionally, several ongoing trials in early-stage TNBC are evaluating various de-escalation strategies. The phase III SCARLET trial (NCT05929768) is comparing a shorter, anthracycline-free chemoimmunotherapy regimen to standard treatment in the neoadjuvant setting, with possible continuation of pembrolizumab post-surgery.39 Cohort I of the phase III ADAPT-TN-IV trial (NCT07178730) is evaluating whether patients with stage II TNBC who achieve a complete clinical response after 12 weeks of neoadjuvant carboplatin/paclitaxel plus pembrolizumab can proceed to surgery, sparing further chemotherapy.40 Earlier trials such as neoADAPT (NCT06245889) and neoTRACT (NCT05645380) are evaluating additional chemoimmunotherapy de-escalation strategies in the neoadjuvant space using imaging and stromal tumor-infiltrating lymphocyte enrichment approaches, respectively.41,42
Figure 1. Examples of Trials Addressing Key Questions in the Optimization of Perioperative ICI-based Treatment Approaches
Logistically, oncology pharmacists can aid in ensuring the appropriate number of cycles are administered in the neoadjuvant and adjuvant settings and that the treatment plan is coordinated with the surgical team, as well as assist with optimal timing of therapy around surgery, as reported in Table 1. Furthermore, should patients complete the protocol-specified neoadjuvant treatment yet have a delay until surgery is scheduled (for reasons not related to toxicity), questions may arise as to whether to continue the ICI while awaiting resection. While not explicitly outlined in the trial protocols, pharmacists can participate in discussions with the care team regarding the benefits and risks of continuing to maintain the scheduled frequency of ICI administration and ensure that the patient ultimately receives the full course of the perioperative regimen. Finally, as data emerges, optimal patient selection, including evaluation of comorbidities and identification of any patient access concerns such as financial toxicity, should be considered when planning to initiate a perioperative ICI-based treatment plan.
As leaders in medication management, oncology pharmacists can provide education to patients and members of the healthcare team regarding anticipated adverse events (AEs) and assist with toxicity monitoring during perioperative treatment. Safety analyses for the combination of an ICI with chemotherapy have not identified any new safety concerns, and AEs have been on par with the known toxicity profiles of each individual therapy, including for immune-related adverse events (irAEs). As data emerges, the benefit of perioperative ICI ought to be weighed against the risk of irAEs, as up to 40% of patients may experience chronic irAEs, including a subset of patients with life-long endocrinopathies and arthritis.33 For targeted therapy, the NeoADAURA trial reported no new safety concerns for perioperative osimertinib alone or with chemotherapy.3 Additionally, treatment-related AEs (TRAEs) were relatively consistent among patients who received chemotherapy with or without an ICI, and importantly, receipt of an ICI did not appear to compromise the ability of patients to undergo surgery.1,13,14,17-24
Conclusion
The treatment landscape for resectable solid tumors continues to evolve rapidly with the use of neoadjuvant or perioperative ICI-based or targeted therapy. The addition of ICIs in the neoadjuvant setting has demonstrated an improvement in pCR for several solid tumors, though how to optimally evaluate response and whether response in this setting translates to long-term survival gains across all malignancies remains to be determined. Additional questions remain as to the benefit of continuing ICIs in the adjuvant setting for those who obtain a pCR or MPR, as well as whether neoadjuvant therapy could be de-escalated. Ideally, future trials will address these questions and better define more personalized approaches to therapy selection in this space by evaluating de-escalation strategies. Oncology pharmacists can continue to enhance patient care by providing education and guidance on optimal implementation of perioperative regimens as data continues to advance.
References
-
Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N Eng J Med. 2020;382:810-821.
-
Puri S, Leighl NB, Ismaila N, et al. Therapy for Stage IV Non-Small Cell Lung Cancer With Driver Alterations: ASCO Living Guideline, 2026.3.0. J Clin Oncol. 2026;44(7):e15-e55.
-
He J, Tsuboi M, Wede W, et al. Neoadjuvant Osimertinib for Resectable EGFR-Mutated Non-Small Cell Lung Cancer. J Clin Oncol. 2025;43(26):2875-2887.
-
Leonetti A, Boni L, Gnetti L, et al. Alectinib as neoadjuvant treatment in potentially resectable stage III ALK-positive NSCLC: final analysis of ALNEO phase II trial (GOIRC-01-2020-ML42316). J Clin Oncol. 2025;43:16s (suppl; abstr 8015).
-
Topalian SL, Forde PM, Emens LA, et al. Neoadjuvant immune checkpoint blockade: A window of opportunity to advance cancer immunotherapy. Cancer Cell. 2023;41(9):1551-1566.
-
Sugiyama K, Gordon A, Popat S, et al. Is pathological response an adequate surrogate marker for survival in neoadjuvant therapy with immune checkpoint inhibitors? ESMO Open. 2025;10(2):104122.
-
Saltalamacchia G, Bernardo A, Quaquarini E, et al. Prognostic Role of Pathological Complete Response in Early Stage Epithelial Solid Tumors. Cancer Control. 2023;30: 10732748231161466.
-
Wei C, Sun H, Hu J, et al. Association of pathological response with long-term survival outcomes after neoadjuvant immunotherapy: A meta-analysis. Int Immunopharmacol. 2024;133:112078.
-
Topalian SL, Taube JM, Pardoll DM. Neoadjuvant checkpoint blockade for cancer immunotherapy. Science. 2020; 367(6477):eaax0182.
-
Mittendorf EA, Burgers F, Haanen J, Cascone T. Neoadjuvant Immunotherapy: Leveraging the Immune System to Treat Early-Stage Disease. Am Soc Clin Oncol Educ Book. 2022;42:1-15.
-
Perioperative Pembrolizumab and Lenvatinib in Resectable Hepatocellular Carcinoma (HCC). ClinicalTrials.gov identifier: NCT05185739. Updated December 6, 2024. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT05185739
-
Perioperative Lenvatinib With Pembrolizumab in Patients With Locally Advanced Nonmetastatic Clear Cell Renal Cell Carcinoma. ClinicalTrials.gov identifier: NCT04393350. Updated February 26, 2025. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT04393350
-
Wakelee H, Liberman M, Kato T, et al. Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N Eng J Med. 2023;389(6):491-503.
-
Heymach JV, Harpole D, Mitsudomi T, et al. Perioperative Durvalumab for Resectable Non-Small-Cell Lung Cancer. N Eng J Med. 2023;389(18):1672-1684.
-
Wu L, Tsuboi M, He J, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Eng J Med. 2020;383(18):1711-1723.
-
A Study of Multiple Therapies in Biomarker-selected Participants With Resectable Stages IB-III Non-small Cell Lung Cancer (NSCLC). ClinicalTrials.gov identifier: NCT04302025. Updated March 6, 2026. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT04302025
-
Cascone T, Awad MA, Spicer JD, et al. Perioperative Nivolumab in Resectable Lung Cancer. N Eng J Med. 2024;390:1756-1769.
-
Blank CU, Lucas MW, Scolver RA, et al. Neoadjuvant Nivolumab and Ipilimumab in Resectable Stage III Melanoma. N Eng J Med. 2024;391(18):1696-1708.
-
Shitara K, Rha SY, Wyrwicz LS, et al. Neoadjuvant and adjuvant pembrolizumab plus chemotherapy in locally advanced gastric or gastro-oesophageal cancer (KEYNOTE-585):an interim analysis of the multicentre, double-blind, randomised phase 3 study. Lancet Oncol. 2024;25(2):212-224.
-
Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Eng J M ed. 2024;391:1773-1786.
-
Uppaluri R, Haddad RI, Tao Y, et al. Neoadjuvant and Adjuvant Pembrolizumab in Locally Advanced Head and Neck Cancer. N Eng J Med. 2025;393:37-50.
-
Janjigian YY, Al-Batran S, Wainberg ZA, et al. Perioperative Durvalumab in Gastric and Gastroesophageal Junction Cancer. N Eng J Med. 2025;393:217-230.
-
Vulsteke C, Adra N, Danchaivijitr P, et al. Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer. N Eng J Med. 2026;[epub ahead of print].
-
Galsky MD, Valderrama BP, Maruzzo M, et al. Neoadjuvant and adjuvant enfortumab vedotin (EV) plus pembrolizumab (pembro) for participants with muscle-invasive bladder cancer (MIBC) who are eligible for cisplatin: randomized, open-label, phase 3 KEYNOTE-B15 study. J Clin Oncol. 2026;44(suppl 7):LBA630. doi:10.1200/JCO.2026.44.7_suppl.LBA630
-
Ruchalski K, Braschi-Amirfarzan M, Douek M, et al. A Primer on RECIST 1.1 for Oncologic Imaging in Clinical Drug Trials. Radiol Imaging Cancer. 2021;3(3):e210008.
-
Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164-172.
-
Rosner S, Liu C, Forde PM, Hu C. Association of pathologic complete response and long-term survival outcomes among patients treated with neoadjuvant chemotherapy or chemoradiotherapy for NSCLC: a meta-analysis. JTO Clin Res Rep. 2022;3(9):100384.
-
Maas M, Nelemans PJ, Valentini V, et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data. Lancet Oncol. 2010;11(9):835-844.
-
Shitara K, Rha SY, Wyrwicz L, et al. Pembrolizumab Plus Chemotherapy Versus Chemotherapy as Perioperative Therapy in Locally Advanced Gastric and Gastroesophageal Junction Cancer: Final Analysis of the Randomized, Phase III KEYNOTE-585 Study. J Clin Oncol. 2025;43:3152-3159.
-
Schmid P, Cortes J, Dent R, et al. Event-free Survival with Pembrolizumab in Early Triple-Negative Breast Cancer. N Eng J Med. 2022;386:556-567.
-
Deutsch JS, Scolyer RA, Burton E, et al. Updated pan-tumor guidelines for neoadjuvant scoring of pathologic response: a joint SITC and INMC effort. Ann Oncol. 2026;37(2):141-154.
-
Deutsch JS, Cimino-Mathews A, Thompson E, et al. Association between pathologic response and survival after neoadjuvant therapy in lung cancer. Nat Med. 2024;30(1):218-228.
-
Johnson DB, Nassar AH, Aijaz A, et al. Reconsidering adjuvant and perioperative immune-checkpoint inhibition: de-escalation, expansion, and personalization. Nat Rev Clin Oncol. 2026;[epub ahead of print].
-
Forde, P. M. et al. Overall survival with neoadjuvant nivolumab plus chemotherapy in lung cancer. N. Engl. J. Med. 2025;393: 741–752.
-
Schmid S, Dimopoulou G, van Schil PE, et al. 175TiP: ETOP 25-23 ADOPT-lung: An international, multicentre, open-label randomised phase III trial to evaluate the benefit of adding adjuvant durvalumab after neoadjuvant chemotherapy plus durvalumab in patients with stage IIB-IIIB (N2) resectable NSCLC. J Thorac Oncol. 2025;20(3):S118 - S119.
-
Immunotherapy After Surgery for People Who Have No Remaining Cancer Cells After Standard Treatment for Early-Stage Non-Small Cell Lung Cancer, INSIGHT Trial. ClinicalTrials.gov identifier: NCT06498635. Updated March 31, 2026. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT06498635
-
Pembrolizumab vs. Observation in People With Triple-negative Breast Cancer Who Had a Pathologic Complete Response After Chemotherapy Plus Pembrolizumab. ClinicalTrials.gov identifier: NCT05812807. Updated March 4, 2026. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT05812807
-
Personalizing the Use of Pembrolizumab for Patients Who Have a Strong Response in Early Triple Negative Breast Cancer (OPT-PEMBRO). ClinicalTrials.gov identifier: NCT06606730. Updated August 26, 2025. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT06606730
-
Shorter Chemo-Immunotherapy Without Anthracycline Drugs for Early-Stage Triple Negative Breast Cancer. ClinicalTrials.gov identifier: NCT05929768. Updated November 5, 2025. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT05929768
-
NeoAdjuvant Therapy Comparing Sacituzumab Govitecan+Pembrolizumab vs. SoC Chemotherapy in Clinical Stage II-III, Triple-negative Early Breast Cancer (ADAPT-TN-IV). ClinicalTrials.gov identifier: NCT07178730. Updated September 17, 2025. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT07178730
-
PET Dynamics to Response-Adapted Neoadjuvant Therapy in TNBC (NeoADAPT). ClinicalTrials.gov identifier: NCT06245889. Updated September 23, 2025. Accessed March 31, 2026. https://clinicaltrials.gov/study/NCT06245889
-
Stecklein SR, Aripoli A, Salgado R, et al. NeoTRACT: Phase II trial of neoadjuvant tumor infiltrating lymphocyte- and response-adapted chemoimmunotherapy for triple-negative breast cancer (TNBC). J Clin Oncol. 2024;42:TPS629-TPS629.


