
Abstract
Background
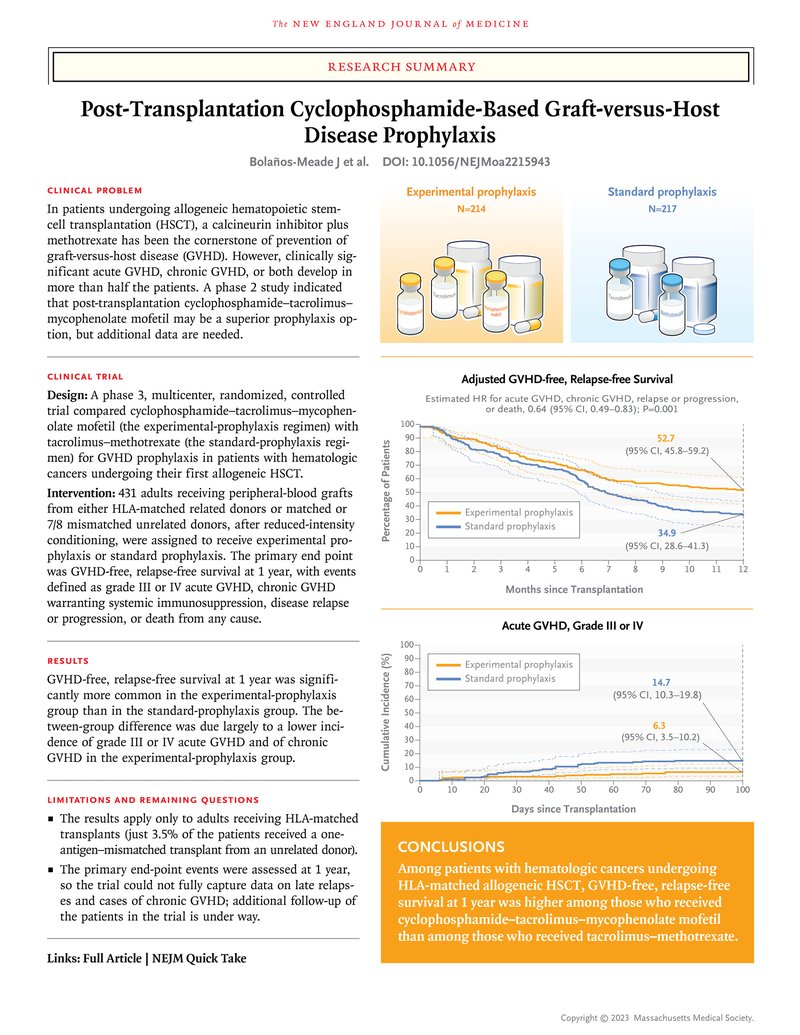
In patients undergoing allogeneic hematopoietic stem-cell transplantation (HSCT), a calcineurin inhibitor plus methotrexate has been a standard prophylaxis against graft-versus-host disease (GVHD). A phase 2 study indicated the potential superiority of a post-transplantation regimen of cyclophosphamide, tacrolimus, and mycophenolate mofetil.
Methods
In a phase 3 trial, we randomly assigned adults with hematologic cancers in a 1:1 ratio to receive cyclophosphamide–tacrolimus–mycophenolate mofetil (experimental prophylaxis) or tacrolimus–methotrexate (standard prophylaxis). The patients underwent HSCT from an HLA-matched related donor or a matched or 7/8 mismatched (i.e., mismatched at only one of the HLA-A, HLA-B, HLA-C, and HLA-DRB1 loci) unrelated donor, after reduced-intensity conditioning. The primary end point was GVHD-free, relapse-free survival at 1 year, assessed in a time-to-event analysis, with events defined as grade III or IV acute GVHD, chronic GVHD warranting systemic immunosuppression, disease relapse or progression, and death from any cause.
Results
In a multivariate Cox regression analysis, GVHD-free, relapse-free survival was significantly more common among the 214 patients in the experimental-prophylaxis group than among the 217 patients in the standard-prophylaxis group (hazard ratio for grade III or IV acute GVHD, chronic GVHD, disease relapse or progression, or death, 0.64; 95% confidence interval [CI], 0.49 to 0.83; P=0.001). At 1 year, the adjusted GVHD-free, relapse-free survival was 52.7% (95% CI, 45.8 to 59.2) with experimental prophylaxis and 34.9% (95% CI, 28.6 to 41.3) with standard prophylaxis. Patients in the experimental-prophylaxis group appeared to have less severe acute or chronic GVHD and a higher incidence of immunosuppression-free survival at 1 year. Overall and disease-free survival, relapse, transplantation-related death, and engraftment did not differ substantially between the groups.
Conclusions
Among patients undergoing allogeneic HLA-matched HSCT with reduced-intensity conditioning, GVHD-free, relapse-free survival at 1 year was significantly more common among those who received cyclophosphamide–tacrolimus–mycophenolate mofetil than among those who received tacrolimus–methotrexate. (Funded by the National Heart, Lung, and Blood Institute and others; BMT CTN 1703 ClinicalTrials.gov number, NCT03959241. opens in new tab.)
Control of graft-versus-host disease (GVHD) is critical for the success of allogeneic hematopoietic stem-cell transplantation (HSCT). Nearly 40 years ago, the combination of methotrexate and a calcineurin inhibitor became the cornerstone for prevention of GVHD; little has changed since then.1 However, despite prophylaxis, clinically significant acute GVHD, chronic GVHD, or both develop in more than half the patients undergoing allogeneic transplantation, and these conditions cause clinically significant complications and death.2-5
In studies conducted over the past half century, high-dose cyclophosphamide spared hematopoietic stem cells and limited GVHD when administered after transplantation.6-8 These observations led to a clinical phase 1–2 trial in which post-transplantation cyclophosphamide–tacrolimus–mycophenolate mofetil was used as GVHD prophylaxis in haploidentical transplantation, and this trial provided a proof of principle.9 The acceptable incidence of GVHD, particularly severe chronic GVHD, was subsequently confirmed in multicenter trials, including those involving patients receiving HLA-mismatched, unrelated donor transplants.10-16
In 2013, the Blood and Marrow Transplant Clinical Trials Network (BMT CTN) launched a phase 2 clinical trial (BMT CTN 1203) comparing three different GVHD prophylaxis strategies with a contemporaneous control regimen of tacrolimus–methotrexate in patients undergoing HSCT after reduced-intensity conditioning.17 The regimens included cyclophosphamide–tacrolimus–mycophenolate mofetil, tacrolimus–methotrexate with bortezomib, and tacrolimus–methotrexate with maraviroc. The trial used a composite primary end point (GVHD-free, relapse-free survival), which was defined as the occurrence of any of the following events from the time of transplantation — grade III or IV acute GVHD, chronic GVHD warranting systemic immunosuppression, disease relapse or progression, or death from any cause — assessed in a time-to-event analysis. That trial identified cyclophosphamide–tacrolimus–mycophenolate mofetil as the most promising regimen to be compared with tacrolimus–methotrexate in a randomized phase 3 trial. Here, we present the results of that phase 3 trial (BMT CTN 1703).
Methods
Trial Design
This randomized, multicenter trial compared two GVHD prophylaxis regimens: cyclophosphamide–tacrolimus–mycophenolate mofetil (experimental prophylaxis) and tacrolimus–methotrexate (standard prophylaxis) in patients receiving reduced-intensity or nonmyeloablative peripheral-blood allogeneic HSCT.18 The primary objective was to compare 1-year GVHD-free, relapse-free survival in the two prophylaxis groups. An event for this time-to-event analysis was defined as grade III or IV acute GVHD, chronic GVHD warranting systemic immune suppression (new systemic immunosuppression in patients with chronic GVHD or continuation of prophylaxis beyond day 180 in patients with active GVHD), disease relapse or progression, or death from any cause by 1 year.
The protocol, available with the full text of this article at NEJM.org, was approved by the institutional review board of the National Marrow Donor Program, and all the patients provided written informed consent. The trial was funded by the National Heart, Lung, and Blood Institute and the National Cancer Institute. The authors vouch for the completeness and accuracy of the data and for the fidelity of the trial to the protocol. No one who is not an author contributed to the writing of the manuscript.
Patients
We planned to enroll 428 eligible patients (214 per group) who were at least 18 years of age and were undergoing their first allogeneic transplantation with the use of peripheral-blood grafts from either unrelated or matched sibling donors after reduced-intensity conditioning. Eligible diagnoses were the following: acute leukemia or chronic myeloid leukemia with no circulating blasts and less than 5% blasts in the bone marrow or myelodysplasia or chronic myelomonocytic leukemia with no circulating blasts and fewer than 10% blasts in the bone marrow, chronic lymphocytic leukemia or small lymphocytic lymphoma, or lymphomas that were sensitive to therapy. Sibling donors were a 6/6 match for HLA-A and HLA-B at intermediate or higher resolution and for DRB1 alleles at high resolution on DNA-based typing, were willing to donate mobilized peripheral blood, and met institutional criteria for donation. Unrelated donors were 7/8 (i.e., mismatched at only one of the HLA-A, HLA-B, HLA-C, and HLA-DRB1 loci) or 8/8 matched at HLA-A, HLA-B, HLA-C, and HLA-DRB1 at high resolution on DNA-based typing, were willing to donate mobilized peripheral blood, and were medically eligible to donate cells according to National Marrow Donor Program criteria.
Treatment
Patients received one of the following reduced-intensity conditioning regimens: fludarabine (120 to 180 mg per square meter of body-surface area) and busulfan (≤8 mg per kilogram of body weight orally or 6.4 mg per kilogram intravenously); fludarabine (120 to 180 mg per square meter) and melphalan (≤150 mg per square meter); fludarabine (90 to 120 mg per square meter) and cyclophosphamide (120 mg per kilogram or 2250 mg per square meter); fludarabine (90 mg per square meter) and total-body irradiation (200 cGy); or fludarabine (150 mg per square meter), total-body irradiation (200 cGy), and cyclophosphamide (29 to 50 mg per kilogram). The target CD34+ cell dose was between 2 and 10×106 per kilogram of actual body weight.
The experimental-prophylaxis regimen consisted of the following: cyclophosphamide (50 mg per kilogram per day on days 3 and 4 after HSCT) with mesna and hydration (details are provided in the protocol); tacrolimus starting on day 5 (in accordance with institutional practices, orally at a dose of 0.05 to 0.06 mg per kilogram per day or intravenously at a dose of 0.02 to 0.03 mg per kilogram per day; taper could start on day 90 with a goal of discontinuation by day 180); and mycophenolate mofetil (15 mg per kilogram per dose orally or intravenously), not to exceed 1 g thrice daily, starting on day 5 to day 35. The standard-prophylaxis regimen consisted of methotrexate (an intravenous bolus of 15 mg per square meter on day 1 and an intravenous bolus of 10 mg per square meter on days 3, 6, and 11) and tacrolimus (dose as above, starting 3 days before HSCT; taper could start on day 90 with a goal of discontinuation by day 180). In both groups, supportive care (antimicrobial prophylaxis and the use of growth factor) was provided according to institutional practice at each center.
End Points
The primary end point was GVHD-free, relapse-free survival at 1 year. Secondary end points were the following: the cumulative incidence of grades II to IV GVHD and of grade III or IV acute GVHD, as defined by the Mount Sinai Acute GVHD International Consortium19; chronic GVHD20; systemic immunosuppression-free survival; hematologic recovery; engraftment; disease relapse or progression; transplantation-related death; disease-free survival; overall survival; post-transplantation lymphoproliferative disorders; infections; and other grade 3 to 5 toxic effects.
Statistical Analysis
Patients were randomly assigned in a 1:1 ratio to the experimental-prophylaxis group or to the standard-prophylaxis group with the use of permuted blocks of random size, stratified according to center and the Disease Risk Index (low, intermediate, or high or very high).21 A two-sided significance level of 0.05 was used to test the null hypothesis of no between-group difference in 1-year GVHD-free, relapse-free survival (the primary end point). In this analysis, we compared the two treatment groups in the intention-to-treat population (all the patients who underwent randomization) using a multivariable Cox regression model adjusted for the following covariates: age, Disease Risk Index, planned regimen, donor type and HLA matching, and planned use of post-transplantation maintenance therapy (declared at the time of enrollment before randomization).
The target sample size of 428 patients (214 per group) was selected to provide the trial with 90% power for a two-sided test to detect a hazard ratio of 0.66 for the experimental-prophylaxis regimen as compared with the standard-prophylaxis regimen, corresponding to 244 total events (grade III or IV acute GVHD, chronic GVHD requiring immune suppressive therapy, relapse or progression or death). This effect size was chosen on the basis of the probabilities of GVHD-free, relapse-free survival observed in the BMT CTN 1203 trial. We estimated an accrual period of 36 months and a 12-month follow-up period with a 5% dropout rate. The trial included one interim efficacy analysis by the National Heart, Lung, and Blood Institute–appointed data and safety monitoring board after 147 events had occurred (60% information fraction) in all evaluable patients. Efficacy stopping rules were based on a unified family design with the shape parameters P=1.44, A=0, R=0, and G=1.9618.22 Point estimates and 95% confidence intervals were constructed for the hazard ratio and for Cox model–adjusted GVHD-free, relapse-free survival at 1 year.23
Figure 1. Randomization, Treatment, and Follow-up.
Analyses with regard to the secondary end points involved only the 420 patients who had received a transplant (the transplantation population) (Figure 1). Overall and disease-free survival were estimated with the use of Cox model–adjusted survival curves for each group. Acute and chronic GVHD, disease relapse, hematologic recovery, and infections were analyzed as competing risks, with death as the competing event for each. Transplantation-related death was analyzed as a competing risk, with relapse or progression as the competing event. To summarize cumulative incidence, we used the Aalen–Johansen estimator and 95% confidence intervals. For the estimates of the cumulative incidence of secondary end-point events, 95% confidence intervals are provided that have not been adjusted for multiplicity and should not be used for hypothesis testing. Proportionality was checked for Cox models with the use of the supremum test for proportional-hazards assumption.24 Simultaneous 95% confidence bands were constructed for adjusted survival and cumulative-incidence curves.25
Other end points were summarized with the use of descriptive statistics. Two unplanned subgroup analyses were performed to further assess the effect of two covariates included in the primary regression model — recipient age and donor type — on the relative hazard of grade III or IV acute GVHD, chronic GVHD, disease relapse or progression, or death with the experimental-prophylaxis regimen as compared with the standard-prophylaxis regimen. Results are derived from post hoc analyses and should be viewed as exploratory only.
Results
Patients
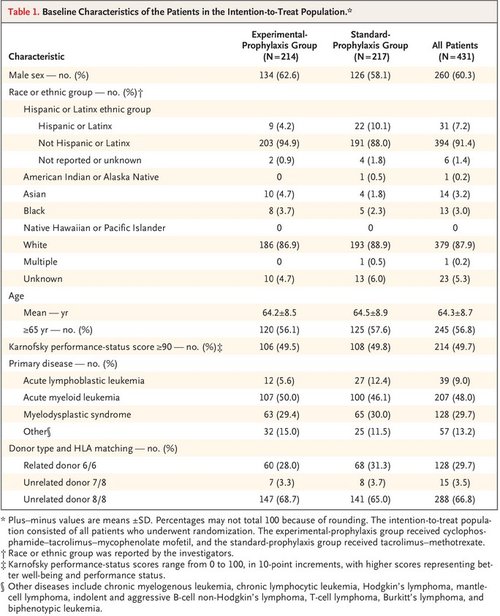
Table 1. Baseline Characteristics of the Patients in the Intention-to-Treat Population.
Between June 25, 2019, and June 18, 2021, a total of 431 patients from 37 centers in the United States were enrolled in the trial (Table 1, and Table S1 in the Supplementary Appendix, available at NEJM.org). Six patients in the experimental-prophylaxis group and 5 in the standard-prophylaxis group did not receive a transplant (Figure 1). The database lock took place on September 19, 2022, for the final analysis. Despite the coronavirus disease 2019 pandemic, the trial completed accrual nearly 1 year ahead of schedule. Table 1 shows the baseline characteristics of the patients (other details are provided in Tables S2 and S3); the two groups were well balanced. The enrolled patients were representative of the general population of HSCT recipients who were the focus of this trial (Table S4). Figure 1 shows randomization, treatment, and follow-up. The median follow-up time for surviving patients was 12 months after randomization (range, 0.2 to 12.0; interquartile range, 12.0 to 12.0). Only 20 patients who were alive at last contact were observed for fewer than 12 months owing to withdrawal, loss to follow-up, or another reason. Data on treatment adherence are provided in Table S5.
Primary End Point
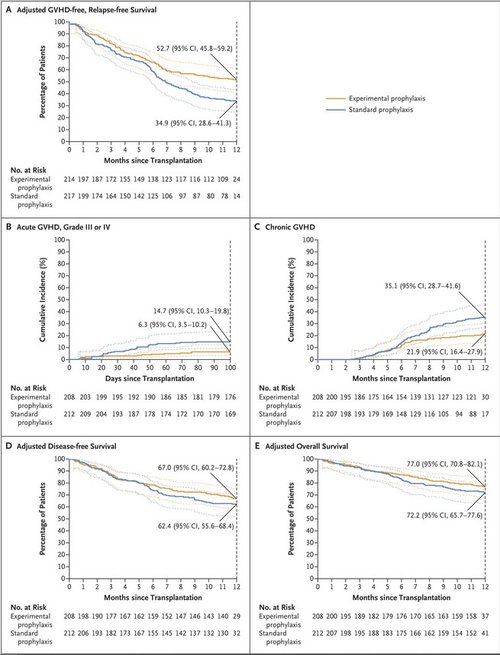
Figure 2. Adjusted Survival Probabilities and the Cumulative Incidence of Primary and Secondary End-Point Events.
The primary analysis was a comparison of the treatment groups in the intention-to-treat population. A total of 233 primary end-point events (98 in the experimental-prophylaxis group and 135 in the standard-prophylaxis group) were observed. A multivariate Cox regression model showed a significantly lower hazard of grade III or IV acute GVHD, chronic GVHD, disease relapse or progression, or death with the experimental-prophylaxis regimen than with the standard-prophylaxis regimen (estimated hazard ratio, 0.64; 95% confidence interval [CI], 0.49 to 0.83; P=0.001). At 1 year, the adjusted GVHD-free, relapse-free survival was 52.7% (95% CI, 45.8 to 59.2) in the experimental-prophylaxis group and 34.9% (95% CI, 28.6 to 41.3) in the standard-prophylaxis group (Figure 2A).
Major Secondary End Points
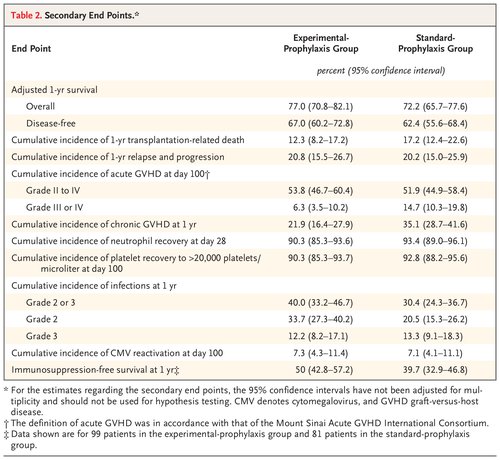
Table 2. Secondary End Points.
Table 2 summarizes the results with respect to the secondary end points. Estimated 1-year overall survival, disease-free survival, and the incidence of transplantation-related death were similar in the two groups. The cumulative incidence of grade II to IV acute GVHD at day 100 was similar in the two groups; however, the estimated cumulative incidence of grade III or IV acute GVHD appeared to be lower in the experimental-prophylaxis group (6.3%; 95% CI, 3.5 to 10.2) than in the standard-prophylaxis group (14.7%; 95% CI, 10.3 to 19.8) (Figure 2B, and Tables S6, S7, and S8). The observed cumulative incidence of chronic GVHD at 12 months after transplantation also favored the experimental-prophylaxis regimen (21.9% [95% CI, 16.4 to 27.9] vs. 35.1% [95% CI, 28.7 to 41.6]) (Figure 2C).
The maximum severity of chronic GVHD through 12 months after transplantation was assessed according to the National Institutes of Health Consensus Development Project Criteria for the grading of chronic GVHD. In the experimental-prophylaxis group, 164 patients did not have chronic GVHD; among those with chronic GVHD, the maximum severity was mild in 29, moderate in 11, and severe in 3 (Table S9). In the standard-prophylaxis group, 139 patients did not have chronic GVDH; among those with chronic GVHD, the maximum severity was mild in 36, moderate in 24, and severe in 11. Immunosuppression-free survival (i.e., patients were alive, did not have relapse, and were not receiving immunosuppression) at 1 year after transplantation appeared to be higher in the experimental-prophylaxis group (50%; 95% CI, 42.8 to 57.2) than in the standard-prophylaxis group (39.7%; 95% CI, 32.9 to 46.8). The median time to neutrophil recovery was 16 days in both groups, although the cumulative incidence of neutrophil recovery at day 28 appeared to be lower in the experimental-prophylaxis group (90.3%; 95% CI, 85.3 to 93.6) than in the standard-prophylaxis group (93.4%; 95% CI, 89.0 to 96.1) and the cumulative incidence of platelet recovery to more than 20,000 platelets per microliter at day 100 appeared to be lower in the experimental-prophylaxis group (90.3%; 95% CI, 85.3 to 93.7) than in the standard-prophylaxis group (92.8%; 95% CI, 88.2 to 95.6). Chimerism at day 100 was similar in the two groups (Table S10).
A total of 489 infections within the first year after randomization were reported by 209 patients (49.8%): 109 of the 208 patients in the experimental-prophylaxis group who underwent transplantation (52.4%) and 100 of the 212 patients in the standard-prophylaxis group who underwent transplantation (47.2%) (Tables S11, S12, and S13). The estimated incidence of grade 2 or 3 infection at 1 year after transplantation was 40.0% (95% CI, 33.2 to 46.7) in the experimental-prophylaxis group and 30.4% (95% CI, 24.3 to 36.7) in the standard-prophylaxis group. The between-group difference was attributable to grade 2 rather than grade 3 infections. The cumulative incidence of cytomegalovirus reactivation at 100 days after transplantation was 7.3% (95% CI, 4.3 to 11.4) in the experimental-prophylaxis group and 7.1% (95% CI, 4.1 to 11.1) in the standard-prophylaxis group. Table S14 summarizes other toxic effects.
The maximum severity of chronic GVHD through 12 months after transplantation was assessed according to the National Institutes of Health Consensus Development Project Criteria for the grading of chronic GVHD. In the experimental-prophylaxis group, 164 patients did not have chronic GVHD; among those with chronic GVHD, the maximum severity was mild in 29, moderate in 11, and severe in 3 (Table S9). In the standard-prophylaxis group, 139 patients did not have chronic GVDH; among those with chronic GVHD, the maximum severity was mild in 36, moderate in 24, and severe in 11. Immunosuppression-free survival (i.e., patients were alive, did not have relapse, and were not receiving immunosuppression) at 1 year after transplantation appeared to be higher in the experimental-prophylaxis group (50%; 95% CI, 42.8 to 57.2) than in the standard-prophylaxis group (39.7%; 95% CI, 32.9 to 46.8). The median time to neutrophil recovery was 16 days in both groups, although the cumulative incidence of neutrophil recovery at day 28 appeared to be lower in the experimental-prophylaxis group (90.3%; 95% CI, 85.3 to 93.6) than in the standard-prophylaxis group (93.4%; 95% CI, 89.0 to 96.1) and the cumulative incidence of platelet recovery to more than 20,000 platelets per microliter at day 100 appeared to be lower in the experimental-prophylaxis group (90.3%; 95% CI, 85.3 to 93.7) than in the standard-prophylaxis group (92.8%; 95% CI, 88.2 to 95.6). Chimerism at day 100 was similar in the two groups (Table S10).
A total of 489 infections within the first year after randomization were reported by 209 patients (49.8%): 109 of the 208 patients in the experimental-prophylaxis group who underwent transplantation (52.4%) and 100 of the 212 patients in the standard-prophylaxis group who underwent transplantation (47.2%) (Tables S11, S12, and S13). The estimated incidence of grade 2 or 3 infection at 1 year after transplantation was 40.0% (95% CI, 33.2 to 46.7) in the experimental-prophylaxis group and 30.4% (95% CI, 24.3 to 36.7) in the standard-prophylaxis group. The between-group difference was attributable to grade 2 rather than grade 3 infections. The cumulative incidence of cytomegalovirus reactivation at 100 days after transplantation was 7.3% (95% CI, 4.3 to 11.4) in the experimental-prophylaxis group and 7.1% (95% CI, 4.1 to 11.1) in the standard-prophylaxis group. Table S14 summarizes other toxic effects.
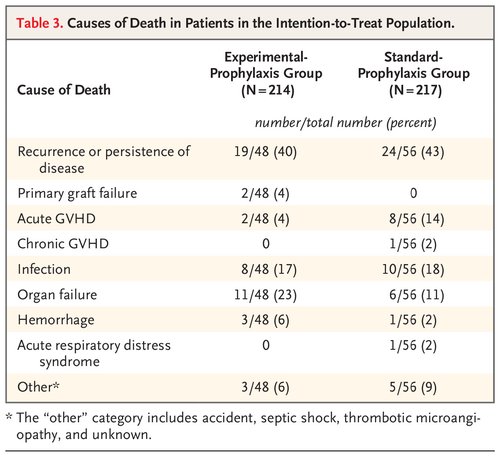
The cumulative incidence of relapse and of progression at 1 year was 20.8% (95% CI, 15.5 to 26.7) in the experimental-prophylaxis group and 20.2% (95% CI, 15.0 to 25.9) in the standard-prophylaxis group. The estimated hazard ratio for relapse was 0.98 (95% CI, 0.64 to 1.52). A total of 55 patients in the experimental-prophylaxis group and 47 patients in the standard-prophylaxis group received post-transplantation therapy to prevent relapse. Epstein–Barr virus–positive lymphoproliferative disorder developed in 1 patient in the experimental-prophylaxis group 308 days after transplantation. Table 3 shows causes of death in the patients in the intention-to-treat population (Table S15).
Other Analyses
Although it was not prespecified in the protocol, a post hoc analysis was performed. That analysis showed similar outcomes in patients who were 65 years of age or older and those who were younger than 65 years of age and in patients who received related donor grafts and those who received unrelated donor grafts (Table S16).
Discussion
This phase 3, randomized trial showed that cyclophosphamide–tacrolimus–mycophenolate mofetil was superior to tacrolimus–methotrexate with respect to GVHD-free, relapse-free survival. This benefit resulted from a decrease in both grade III or IV acute GVHD and chronic GVHD and was accompanied by increased estimated immunosuppression-free survival. Despite the decreased incidence of GVHD, there were no substantial changes in relapse, engraftment, hematopoietic recovery, transplantation-related death, severe infections, or overall survival. These findings are remarkable because more aggressive GVHD control has historically been associated with a higher incidence of relapse and worse overall outcomes.26 Patients in the experimental-prophylaxis group had a longer time to platelet recovery and a higher incidence of grade 2 infections than those in the standard-prophylaxis group, although this did not adversely affect GVHD-free, relapse-free survival or overall survival.
Previous, smaller trials have compared cyclophosphamide-based GVHD prophylaxis with calcineurin inhibitor–based GVHD prophylaxis. In particular, the randomized, phase 2, BMT CTN 1203 trial compared three different prophylaxis regimens, one of which was cyclophosphamide–tacrolimus–mycophenolate mofetil. Each group was compared with a nonrandomized but contemporaneous control group of patients receiving tacrolimus–methotrexate, whose data had been reported to the Center for International Blood and Marrow Transplant Research (CIBMTR) registry.17 In that trial, cyclophosphamide–tacrolimus–mycophenolate mofetil was associated with the best results of the three experimental groups and was the only regimen that was superior to the control regimen. Consequently, the BMT CTN decided to proceed with the current phase 3 trial.
The phase 3 Dutch–Belgian Cooperative Trial Group for Hematology–Oncology (HOVON) 96 trial compared cyclophosphamide and cyclosporine with mycophenolic acid and cyclosporine after transplantation with reduced-intensity conditioning. However, the cyclophosphamide group was added in a fourth amendment to the protocol without modification or adaption of the primary end point (severe GVHD at 6 months).27 The HOVON-96 trial showed that cyclophosphamide was superior to cyclosporine and mycophenolic acid with respect to GVHD-free, relapse-free survival at 1 year among 99 patients and 52 patients, respectively (45% vs. 21%; P<0.001), with no negative effect on overall or disease-free survival. Other differences are noted between the HOVON-96 trial and the current BMT CTN 1703 trial. The combination of mycophenolic acid and cyclosporine used in the HOVON-96 trial has not been tested in other phase 3 studies of GVHD, to our knowledge. Data from the CIBMTR suggest that the combination of mycophenolate mofetil and cyclosporine led to outcomes with respect to GVHD and overall survival that were inferior to those with tacrolimus–methotrexate after HSCT from an unrelated donor and reduced-intensity conditioning.28 The HOVON-96 trial did not use the widely used cyclophosphamide–tacrolimus–mycophenolate mofetil regimen developed at Johns Hopkins University School of Medicine, but rather cyclophosphamide and cyclosporine; the effects of eliminating mycophenolate mofetil from the regimen are unknown.
Finally, cyclosporine is not the current standard of care for GVHD prophylaxis in the United States; it is used in fewer than 10% of HLA-matched transplantations with reduced-intensity conditioning. In contrast, tacrolimus is used in more than 70% of such procedures (CIBMTR data). The current trial provides strong evidence of the superiority of cyclophosphamide–tacrolimus–mycophenolate mofetil over the most commonly used GVHD prophylaxis regimen for HLA-matched transplantation in the United States. Cyclophosphamide–tacrolimus–mycophenolate mofetil has also been used after myeloablative conditioning, but comparisons of this regimen with tacrolimus–methotrexate are lacking.29-31
Of note, the median age in our trial was 66 years. Until recently, many centers would not have permitted patients 65 years of age or older to undergo transplantation. In the current trial, results of post hoc analyses suggest similar outcomes in patients who were 65 years of age or older and those who were younger than 65 years of age in both groups; these findings suggest overall advances in the use of supportive care in addition to GVHD prophylaxis that afford access to older patients.
Although cyclophosphamide–tacrolimus–mycophenolate mofetil has been used in children, our data apply only to adults receiving HLA-matched transplants.32 In addition, although the trial allowed unrelated one-antigen mismatches, few patients had such donors (only 3.5%). However, other studies have shown cyclophosphamide–tacrolimus–mycophenolate mofetil to be effective in HLA-mismatched, unrelated donor transplantation.14 The trial did not allow the use of antithymocyte globulin, which some studies have shown to be effective in preventing GVHD after myeloablative transplantation.33-35 However, antithymocyte globulin is not commonly used in the United States in patients receiving reduced-intensity conditioning and was specifically avoided in this trial because of its association with an increased incidence of relapse and shorter survival.36,37 Although some concern was expressed that cyclophosphamide might delay immune recovery, and a higher overall incidence of infections was noted in the cyclophosphamide–tacrolimus–mycophenolate mofetil group, only one case of post-transplantation lymphoproliferative disorder was documented, and the two groups had a similar incidence of cytomegalovirus reactivations and grade 3 infections. Finally, many of the end-point events were assessed at 1 year, and data on late relapses and cases of chronic GVHD were thus not fully captured as late complications. Continued follow-up of these cohorts is under way.
In this trial, patients who received cyclophosphamide–tacrolimus–mycophenolate mofetil had longer GVHD-free, relapse-free survival than those who received tacrolimus–methotrexate. The results also suggested longer immunosuppression-free survival and a lower incidence of severe acute GVHD and of chronic GVHD with the experimental-prophylaxis regimen, without an early (≤1 year) compromise in disease control, although these results require confirmation.
Supported by grants (U10HL069294 and U24HL138660, to Dr. Horowitz) from the National Heart, Lung, and Blood Institute (NHLBI) and the National Cancer Institute (NCI); a grant (U24-CA76518, to the Center for International Blood and Marrow Transplant Research [CIBMTR]) from the NCI, the NHLBI, and the National Institute of Allergy and Infectious Diseases; and by a contract (HHSH234200637015C, to the CIBMTR) from the Health Resources and Services Administration and the Department of Health and Human Services.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
A data sharing statement provided by the authors is available with the full text of this article at NEJM.org.
We thank the National Marrow Donor Program for support and the patients who participated in the trial.
Author Affiliations
From the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University, and the Department of Oncology, Johns Hopkins University School of Medicine, Baltimore (J.B.-M., R.J.J.), Emmes, Rockville (J.W., K.A.), and the Division of Blood Diseases and Resources (N.L.D.) and the Office of Biostatistics Research (E.L.), National Heart, Lung, and Blood Institute, Bethesda — all in Maryland; the Blood and Marrow Transplant Program and Cellular Therapy Program (M.H.) and the Center for International Blood and Marrow Transplant Research (CIBMTR), Department of Medicine (M.H., M.M.H.), the CIBMTR Division of Biostatistics, Institute for Health and Equity (M.J.M.), and the Division of Hematology and Oncology, Department of Medicine (L.R.), Medical College of Wisconsin, Milwaukee, and the Division of Hematology and Oncology, Department of Medicine, University of Wisconsin School of Medicine and Public Health, Madison (A.C.H.) — both in Wisconsin; the Division of Blood and Marrow Transplantation and Cellular Therapy, Department of Medicine, Stanford University School of Medicine, Stanford (A.R.R.), the Department of Hematology and Hematopoietic Cell Transplantation, City of Hope (M.M.A.M.), and the Department of Pharmacy, City of Hope National Medical Center (J.M.Y.), Duarte, and the Division of Hematology, Departments of Medicine and Genetics, Stanford University, Palo Alto (A.S.B.) — all in California; the Department of Blood and Marrow Transplant and Cellular Immunotherapy, H. Lee Moffitt Cancer and Research Institute, Tampa, FL (H.E.); the Department of Hematology and Oncology, Dana–Farber Cancer Institute (M.G., L.S.K.), and the Department of Pediatrics, Harvard Medical School, and the Division of Pediatric Hematology and Oncology, Boston Children’s Hospital (L.S.K.) — all in Boston; the Ohio State University Comprehensive Cancer Center, Columbus (K.T.L., Y.A.E.); Adult Bone Marrow Transplantation Service, Memorial Sloan Kettering Cancer Center, and the Department of Medicine, Weill Cornell Medical College (B.C.S., M.-A.P.), and the Blood and Marrow Transplantation Program, Columbia University Irving Medical Center (R.R.) — all in New York; the Division of Hematology, Oncology, and Transplantation, University of Minnesota, Minneapolis (N.E.J., S.G.H.); the Division of Hematology and Oncology, Perelman School of Medicine, University of Pennsylvania, Philadelphia (A.W.L.); the Blood and Marrow Transplant Program at Northside Hospital, Atlanta (M.S.); the Department of Stem Cell Transplantation and Cellular Therapy, the University of Texas M.D. Anderson Cancer Center, Houston (A.M.A.); the Division of Hematology and Oncology, Department of Medicine, University of Alabama at Birmingham, Birmingham (O.H.J.); and the Division of Hematology–Oncology and Palliative Care, Department of Medicine, Virginia Commonwealth University, Richmond (W.C.).
Dr. Bolaños-Meade can be contacted at fbolano2@jhmi.edu or at the Sidney Kimmel Comprehensive Cancer Center, 1650 Orleans St., CRB-I-2M87, Baltimore, MD 21287.
A list of the BMT CTN 1703 Investigators is provided in the Supplementary Appendix, available at NEJM.org.

