
Abstract
Background
Ciltacabtagene autoleucel (cilta-cel), a B-cell maturation antigen (BCMA)–directed CAR T-cell therapy, is effective in heavily pretreated patients with relapsed or refractory multiple myeloma. We investigated cilta-cel in earlier treatment lines in patients with lenalidomide-refractory disease.
Methods
In this phase 3, randomized, open-label trial, we assigned patients with lenalidomide-refractory multiple myeloma to receive cilta-cel or the physician’s choice of effective standard care. All the patients had received one to three previous lines of treatment. The primary outcome was progression-free survival.
Results
A total of 419 patients underwent randomization (208 to receive cilta-cel and 211 to receive standard care). At a median follow-up of 15.9 months (range, 0.1 to 27.3), the median progression-free survival was not reached in the cilta-cel group and was 11.8 months in the standard-care group (hazard ratio, 0.26; 95% confidence interval [CI], 0.18 to 0.38; P<0.001). Progression-free survival at 12 months was 75.9% (95% CI, 69.4 to 81.1) in the cilta-cel group and 48.6% (95% CI, 41.5 to 55.3) in the standard-care group. More patients in the cilta-cel group than in the standard-care group had an overall response (84.6% vs. 67.3%), a complete response or better (73.1% vs. 21.8%), and an absence of minimal residual disease (60.6% vs. 15.6%). Death from any cause was reported in 39 patients and 46 patients, respectively (hazard ratio, 0.78; 95% CI, 0.5 to 1.2). Most patients reported grade 3 or 4 adverse events during treatment. Among the 176 patients who received cilta-cel in the as-treated population, 134 (76.1%) had cytokine release syndrome (grade 3 or 4, 1.1%; no grade 5), 8 (4.5%) had immune effector cell–associated neurotoxicity syndrome (all grade 1 or 2), 1 had movement and neurocognitive symptoms (grade 1), 16 (9.1%) had cranial nerve palsy (grade 2, 8.0%; grade 3, 1.1%), and 5 (2.8%) had CAR-T–related peripheral neuropathy (grade 1 or 2, 2.3%; grade 3, 0.6%).

Conclusions
A single cilta-cel infusion resulted in a lower risk of disease progression or death than standard care in lenalidomide-refractory patients with multiple myeloma who had received one to three previous therapies. (Funded by Janssen and Legend Biotech; CARTITUDE-4 ClinicalTrials.gov number, NCT04181827. opens in new tab.)
Quick Take: Cilta-cel in Lenalidomide-Refractory Multiple Myeloma
Most patients with multiple myeloma have a relapse after standard treatment,1,2 and outcomes worsen with each subsequent line of therapy.3-5 Lenalidomide is an immunomodulator that is recommended6,7 for newly diagnosed and relapsed or refractory multiple myeloma. The use of lenalidomide has become widespread as early-line treatment, including as maintenance therapy.1,8 The frequency of lenalidomide resistance early in the treatment journey is increasing,1,8 which has led to a growing need for new, effective therapies for lenalidomide-refractory disease.8 High treatment attrition — only 13 to 35% of patients receive four or more lines of therapy — also highlights the need to use effective therapies early.9
In early trials, ciltacabtagene autoleucel (cilta-cel), a chimeric antigen receptor T-cell (CAR-T) therapy directed against B-cell maturation antigen (BCMA), led to early, deep, and durable responses in patients with relapsed or refractory multiple myeloma. In the phase 1b–2 CARTITUDE-1 trial involving patients who had received at least three lines of therapy, the median progression-free survival was 34.9 months.10-12 The phase 2 CARTITUDE-2 trial showed the efficacy of cilta-cel in small groups (cohorts A and B) at earlier disease stages, with response rates of 95 to 100% and an estimated duration of response of at least 12 months in 79 to 89% of patients who had a response. After approximately 1.5 years of follow-up, 75 to 90% of patients remained progression-free.13,14 In a phase 3 trial of another CAR-T therapy, idecabtagene vicleucel, involving patients who had received two to four lines of therapy for multiple myeloma, investigators found a median progression-free survival of 13.3 months (hazard ratio, 0.49 as compared with standard treatments).15
We conducted the phase 3 CARTITUDE-4 trial to compare cilta-cel with the physician’s choice of either of two highly effective standard-of-care therapies in patients with lenalidomide-refractory multiple myeloma after one to three lines of therapy. Here, we report the efficacy and safety results from the interim analysis.
Methods
Trial Design and Patients
We conducted this open-label, randomized trial at 81 sites in the United States, Europe, Asia, and Australia. Eligible patients had lenalidomide resistance16 and had received one to three lines of therapy, including a proteasome inhibitor and an immunomodulatory drug. All the patients had an Eastern Cooperative Oncology Group performance-status score of 1 or less (on a scale ranging from 0 to 5, with higher scores indicating greater disability). In addition, none of the patients had received CAR-T therapy or BCMA-targeted treatment. Full eligibility criteria are provided in the protocol, available with the full text of this article at NEJM.org.
Randomization and Treatments
Patients were assigned in a 1:1 ratio by means of computer-generated randomization to receive standard care (physician’s choice of pomalidomide, bortezomib, and dexamethasone [PVd]17 or daratumumab, pomalidomide, and dexamethasone [DPd])18 or a single cilta-cel infusion, administered after the physician’s choice of bridging therapy (PVd or DPd). Randomization was stratified according to the selection of PVd or DPd, disease severity according to the International Staging System (ISS) at screening (I, II, or III), and the number of previous lines of therapy (1 or 2 to 3).
In the standard-care group, DPd was administered in 28-day cycles and PVd in 21-day cycles until disease progression (see the Supplementary Appendix, available at NEJM.org). According to the protocol, if patients had disease progression after standard treatment, crossover from the standard-care group to the cilta-cel group was not permitted. Patients in the cilta-cel group underwent apheresis, followed by at least one bridging therapy cycle (with the number of cycles based on clinical status and cilta-cel manufacturing time) and lymphodepletion (300 mg of cyclophosphamide per square meter of body-surface area and 30 mg of fludarabine per square meter daily for 3 days). Five to seven days after the initiation of lymphodepletion, a single cilta-cel infusion (target dose, 0.75×106 CAR+ viable T cells per kilogram of body weight) was administered. Patients in the cilta-cel group who had confirmed disease progression during bridging therapy or lymphodepletion were assessed as having a progression event and could receive cilta-cel as subsequent therapy at the investigator’s discretion.
Outcomes and Assessments
The primary outcome was progression-free survival, which was defined as the time from randomization to the first documentation of disease progression or death. The key secondary outcomes were sequentially tested in order at each prespecified significance level and included complete response or better, overall response, minimal residual disease (MRD) negativity, overall survival, and worsening of patient-reported symptoms as assessed by the Multiple Myeloma Symptom and Impact Questionnaire. Additional secondary outcomes included adverse events and cilta-cel pharmacokinetics.
Treatment responses and disease progression were determined according to the International Myeloma Working Group criteria16 with the use of a validated computer algorithm.19 Blood and 24-hour urine samples were analyzed at a central laboratory until the confirmation of disease progression. The presence of MRD was assessed centrally by next-generation sequencing (clonoSEQ, version 2.0, Adaptive Biotechnologies) on bone marrow samples at a sensitivity of 1.0×10−5.
Cytokine release syndrome and immune effector cell–associated neurotoxicity syndrome (ICANS) were graded according to consensus criteria of the American Society for Transplantation and Cellular Therapy.20 Other adverse events, including investigator-assessed non-ICANS neurotoxicity, were graded according to the Common Terminology Criteria for Adverse Events of the National Cancer Institute, version 5.0.21
Oversight
The trial was funded by Janssen and Legend Biotech, and representatives of the companies were involved in the collection, analysis, and interpretation of the data. The trial was conducted in accordance with the Declaration of Helsinki and International Council for Harmonisation guidelines for Good Clinical Practice. All patients provided written informed consent. The independent ethics committee or institutional review board at each site approved the trial protocol. A data and safety monitoring committee monitored all safety data collected in the clinical program and evaluated the interim safety and efficacy data (see the Supplementary Appendix).
All the authors contributed to trial conduct, data analyses, and drafting of the manuscript and vouch for the accuracy and completeness of the data and for the fidelity of the trial to the protocol. Medical writing assistance was funded by Janssen Global Services; all drafts were critically reviewed, revised, and approved by the authors.
Statistical Analysis
We estimated that the enrollment of 400 patients and the occurrence of 250 events of disease progression or death would provide the trial with 90% power to detect a relative reduction of 35% in the risk of disease progression or death. This calculation was based on the results of a log-rank test at an overall two-sided alpha level of 0.05, under a group sequential design with one interim analysis to evaluate the primary outcome, a prespecified analysis to be conducted after the occurrence of approximately 188 primary-outcome events. The significance level that was required to establish superiority was determined on the basis of the number of events that were observed, with the use of O’Brien–Fleming boundaries and implemented by the Lan–DeMets alpha-spending method. Details are provided in the Supplementary Appendix.
Efficacy was evaluated in the intention-to-treat population, which included all the patients who had undergone randomization. Adverse events were evaluated in the safety population, which included all the patients who had received any portion of a trial treatment. Adverse events that were specific to CAR-T therapy were evaluated in the as-treated population (patients who had received cilta-cel as the trial treatment).
Progression-free survival was estimated by means of the Kaplan–Meier method. We used a stratified constant piecewise weighted log-rank test (in which a weight of 0 was assigned for the log-rank statistic for weeks 0 to 8 after randomization and a weight of 1 after that period)22,23 to compare the trial groups, because both groups received the same treatments during the bridging period. The hazard ratio and its two-sided 95% confidence intervals were estimated with the use of a stratified Cox regression model with treatment as the sole explanatory variable. We used the Kaplan–Meier method and stratified log-rank tests to analyze other time-to-event outcomes. Binary outcomes were analyzed with the use of stratified Cochran–Mantel–Haenszel tests. The worsening of symptoms was defined as a meaningful increase (estimated by distribution-based methods of at least half a standard deviation of pooled baseline values) without a subsequent reduction in myeloma symptoms.
Results
Patients
From July 10, 2020, through November 17, 2021, a total of 419 patients were randomly assigned to receive cilta-cel (208 patients) or standard care (211 patients). Of the patients in the standard-care group, 183 received DPd and 28 received PVd. All the patients in the cilta-cel group received bridging therapy (DPd in 182 or PVd in 26).
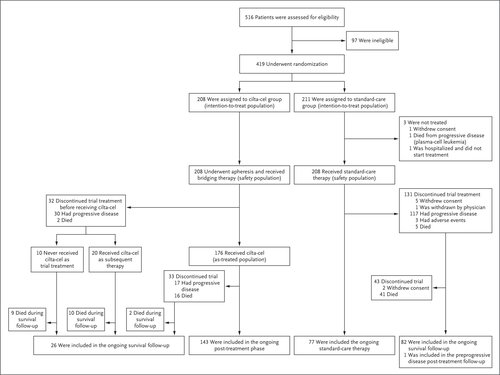
Figure 1. Enrollment and Outcomes.
Of the patients in the cilta-cel group, 176 (84.6%) actually received cilta-cel (as-treated population). The remaining 32 patients discontinued trial participation before receiving cilta-cel, predominantly because of disease progression during bridging therapy or lymphodepletion. Of these patients, 20 received cilta-cel as a subsequent therapy. No patients discontinued a trial treatment because of drug-manufacturing failure. The median time from the receipt of apheresis material to product release was 44 days (range, 25 to 127) (see the Supplementary Appendix). In the standard-care group, 208 patients (98.6%) received the assigned drug; of these patients, 131 (63.0%) discontinued treatment, primarily because of disease progression (in 56.3%) (Figure 1). By the data-cutoff date (November 1, 2022), the median follow-up was 15.9 months (range, 0.1 to 27.3).
The characteristics of the patients were well balanced in the two groups (Table 1). The demographic characteristics largely reflected real-world patients with myeloma (Table S1 in the Supplementary Appendix). High-risk cytogenetic features — del17p, t(4;14), t(14;16), or gain/amp(1q) — were identified in 59.4% of the patients in the cilta-cel group and in 62.9% of those in the standard-care group; at least two high-risk cytogenetic abnormalities were identified in 20.7% and 23.2%, respectively. Soft-tissue plasmacytomas were identified at baseline in 21.2% of the patients in the cilta-cel group and in 16.6% in the standard-care group. In the cilta-cel group, 30 patients (14.4%) had triple-class drug resistance; 50 (24.0%) had resistance to anti-CD38 antibody. The median cilta-cel dose was 0.71×106 cells per kilogram. In the standard-care group, patients received a median of 12 treatment cycles (range, 1 to 28).
Efficacy
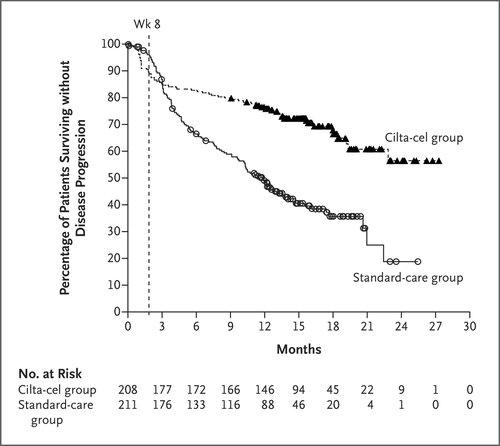
Figure 2. Kaplan–Meier Analysis of Progression-free Survival (Intention-to-Treat Population).
Cilta-cel resulted in a significantly lower risk of disease progression or death than standard care (hazard ratio, 0.26; 95% confidence interval [CI], 0.18 to 0.38; P<0.001). The median duration of progression-free survival was not reached in the cilta-cel group and was 11.8 months (95% CI, 9.7 to 13.8) in the standard-care group (Figure 2). At 12 months in the intention-to-treat population, progression-free survival was 75.9% (95% CI, 69.4 to 81.1) in the cilta-cel group and 48.6% (95% CI, 41.5 to 55.3) in the standard-care group. An unweighted sensitivity analysis showed results that were similar to those in the primary analysis (Table S2). Similar effects were seen in all subgroups of patients, including those with high-risk cytogenetic features, soft-tissue plasmacytomas, triple-class–refractory disease, and other high-risk disease factors, as well as across different numbers of previous lines of therapy (Fig. S1).
During the first 8 weeks after randomization, disease progression or death occurred in 22 patients in the cilta-cel group and in 8 patients in the standard-care group. All these events occurred before the infusion of cilta-cel while patients were receiving the same therapy in the two groups. During the bridging period, patients in the cilta-cel group received doses of pomalidomide and bortezomib that were approximately 14% lower than those in the standard-care group, which could have affected the primary outcome.
Table 2. Treatment Response and Minimal Residual Disease (Intention-to-Treat Population).
More patients in the cilta-cel group than in the standard-care group had a complete response or better (73.1% vs. 21.8%), for a risk ratio of 2.9 (95% CI, 2.3 to 3.7; P<0.001) and an odds ratio of 10.3 (95% CI, 6.5 to 16.4) (Table 2 and the Supplementary Appendix). The overall response (partial response or better) was 84.6% and 67.3%, respectively, for a risk ratio of 2.2 (95% CI, 1.5 to 3.1; P<0.001) and an odds ratio of 3.0 (95% CI, 1.8 to 5.0). Among the patients who had a response, an estimated 84.7% in the cilta-cel group as compared with 63.0% in the standard-care group continued to have a response for at least 12 months.
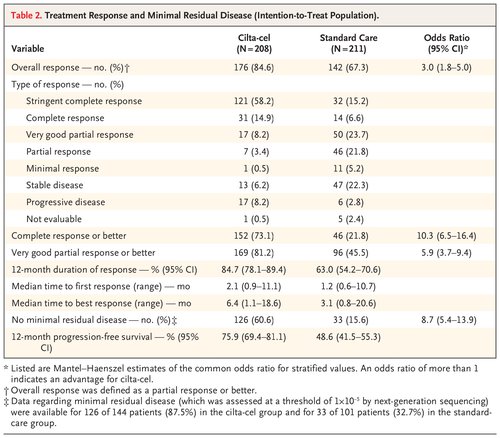
MRD negativity at any time during the trial occurred in 60.6% of the patients in the cilta-cel group and in 15.6% of those in the standard-care group, for a risk ratio of 2.2 (95% CI, 1.8 to 2.6; P<0.001) and an odds ratio of 8.7 (95% CI, 5.4 to 13.9). Among the patients who had evaluable samples (144 in the cilta-cel group and 101 in the standard-care group), MRD negativity occurred in 126 (87.5%) and 33 (32.7%), respectively.
Overall survival data were immature at the time of this report (hazard ratio, 0.78; 95% CI, 0.5 to 1.2; P=0.26). At 12 months, an estimated 84.1% of patients in the cilta-cel group were alive, as compared with 83.6% in the standard-care group.
The median time until symptom worsening was 23.7 months (95% CI, 22.1 to not estimable) in the cilta-cel group and 18.9 months (95% CI, 16.8 to not estimable) in the standard-care group (hazard ratio, 0.42; 95% CI, 0.26 to 0.68). Efficacy results for the 176 patients who received cilta-cel in the as-treated population are provided in Figure S2 and Table S3.
Safety
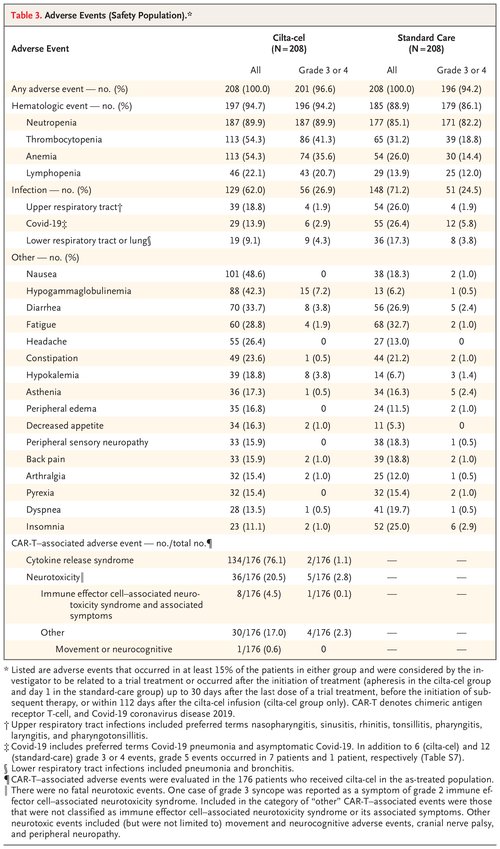
Table 3. Adverse Events (Safety Population).
In the safety population (208 patients in each of the two groups), grade 3 or 4 adverse events occurred in 201 patients (96.6%) in the cilta-cel group and in 196 (94.2%) in the standard-care group (Table 3). The most common grade 3 or 4 adverse events in both groups were hematologic; most high-grade cytopenias in patients who received cilta-cel recovered to grade 2 or less by day 60 (Table S4). Serious adverse events were reported in 92 patients (44.2%) in the cilta-cel group and in 81 (38.9%) in the standard-care group (Table S5). In the standard-care group, 3 patients (1.4%) discontinued treatment and 115 (55.3%) had cycle delays because of adverse events.
Second primary cancers were diagnosed in 9 patients (4.3%) in the cilta-cel group and in 14 (6.7%) in the standard-care group; hematologic and cutaneous or noninvasive cancers were the most common (Table S6).
During treatment, infections occurred in 129 patients (62.0%) in the cilta-cel group and in 148 (71.2%) in the standard-care group; of these infections, 26.9% and 24.5%, respectively, were of grade 3 or 4. Coronavirus disease 2019 (Covid-19) that was considered to have occurred during treatment was diagnosed in 29 patients (13.9%) in the cilta-cel group and in 55 (26.4%) in the standard-care group (Table 3). On the basis of adverse-event reporting and laboratory results, the incidence of hypogammaglobulinemia was 90.9% in the cilta-cel group and 71.6% in the standard-care group; on the basis of adverse-event reporting alone, the corresponding incidence was 42.3% and 6.2%, respectively. A total of 65.9% and 12.5% of patients, respectively, received intravenous immune globulin.
Death from any cause was reported in 39 patients in the cilta-cel group and in 46 in the standard-care group; 1 patient in the standard-care group died before the initiation of treatment. Death from disease progression was reported in 14 patients in the cilta-cel group (8 of whom did not receive cilta-cel) and in 30 in the standard-care group; 10 and 5 deaths, respectively, were caused by adverse events during treatment (associated with Covid-19 in 7 patients and 1 patient, respectively). A total of 15 deaths in the cilta-cel group and 11 deaths in the standard-care group were due to adverse events that were not considered by the investigator to be related to a trial treatment. These deaths occurred after the start of subsequent therapy or more than 112 days after the cilta-cel infusion or more than 30 days after the last dose of a standard-care treatment (Table S7).
Of the 176 patients who received cilta-cel in the as-treated population, 134 (76.1%) had cytokine release syndrome (grade 1 or 2 in 132 and grade 3 in 2). The median time until the onset was 8 days (range, 1 to 23), and the duration was 3 days (range, 1 to 17) (Table S8). CAR-T–related neurotoxic events occurred in 36 patients (20.5%), with grade 1 or 2 in 31 and grade 3 or 4 in 5. All 8 cases of ICANS (4.5%) were of grade 1 or 2, with a median of 9.5 days (range, 6 to 15) until onset and a median duration of 2 days (range, 1 to 6) (Table S9). One episode of movement and neurocognitive adverse events (grade 1) was reported in a male patient with previous grade 2 cytokine release syndrome whose disease was resistant to bridging therapy (Table S10). Onset was on day 85 after infusion and was ongoing at the time of data cutoff. Cranial nerve palsies, which most commonly affected cranial nerve VII, were reported in 16 patients (9.1%) (grade 1 or 2 in 14 and grade 3 in 2), and median onset was 21 days (range, 17 to 60) after infusion; 14 patients had recovered by the time of data cutoff. CAR-T–related peripheral neuropathies were reported in 5 patients (2.8%); 3 had recovered by data cutoff (Table S10).
Cilta-cel Pharmacokinetics
Among the 176 patients in the as-treated population who received cilta-cel, CD3+CAR+ cells in blood peaked at a median of 13 days after infusion; the mean (±SD) number of cells was 1523±5987 per cubic millimeter. These cells remained detectable for a median of 57 days (range, 13 to 631). During the first 28 days after the administration of cilta-cel, the mean area under the curve was 12,504±55,281 CD3+CAR+ cells.
Discussion
In patients with lenalidomide-refractory multiple myeloma after one to three previous lines of therapy, a single cilta-cel infusion resulted in a lower risk of disease progression or death (the primary outcome) than highly effective standard-care treatments (mostly DPd) at a median follow-up of 15.9 months. At 12 months, progression-free survival was 75.9% as compared with 48.6% with standard care. Similar effects were seen in all subgroups that were evaluated, including patients with high-risk cytogenetic abnormalities, soft-tissue plasmacytomas, triple-class–refractory disease, ISS stage III status, and other high-risk features. Moreover, cilta-cel had higher response rates, deeper and more durable responses, and a higher frequency of MRD negativity than standard care; the time until patient-reported worsening of symptoms was complementary to clinical outcomes. These results indicate that cilta-cel is an effective treatment for patients with lenalidomide-refractory disease as early as the first relapse. The results also add to the consistently strong efficacy that cilta-cel has shown throughout its clinical development, including in similar, early lines of therapy populations in CARTITUDE-2,13,14 and confirm the efficacy observed in heavily pretreated patients who received cilta-cel in CARTITUDE-1.10,11
The protocol did not mandate the physician’s choice of standard-care (or bridging) therapy on the basis of previous exposure or resistance to the previous receipt of proteasome inhibitors or daratumumab. However, most patients received DPd, and the standard-care treatments in CARTITUDE-4 performed as expected according to the findings of the APOLLO and OPTIMISMM trials involving patients with multiple myeloma.17,18
A potential limitation of the trial design was that two highly efficacious triplet regimens — daratumumab, carfilzomib, and dexamethasone and isatuximab, carfilzomib, and dexamethasone — were not approved at the time of trial initiation and could not be included as standard-care options. These two regimens have since entered clinical practice as treatment options.24-27 However, the populations in these trials differed from our trial population, and lenalidomide resistance was not a criterion for inclusion.
Patients in our two trial groups received the same medications that were administered during the period of bridging therapy in the cilta-cel group. Thus, a prespecified weighting method was used in the two groups to focus outcomes on events after the cilta-cel infusion. The numbers of progression events or deaths that were reported during trial weeks 0 to 8 — all of which preceded the cilta-cel infusion — were higher in the cilta-cel group than in the standard-care group. This difference may have been due to lower doses of DPd and PVd that were used in the cilta-cel group. The occurrence of these early events meant that the benefit of cilta-cel did not become apparent in the Kaplan–Meier curve for the primary analysis until 3 months.
Understanding the mechanisms of drug resistance is an area of interest that will ultimately assist in the sequencing of myeloma therapies. These analyses are in progress. The median duration of progression-free survival in CARTITUDE-4 extended beyond the median duration of detectability in CAR T cells, a result that was similar to observations in CARTITUDE-1.
Before the clinical cutoff date, 7 deaths related to Covid-19 were documented in the cilta-cel group, of which 6 infections were diagnosed within 4 months after the cilta-cel infusion, when patients were most immunocompromised. Furthermore, the time period coincided with the emergence of the omicron variant and the relaxing of Covid-19–related restrictions in some regions. These deaths contributed to the higher number of fatal events observed in the cilta-cel group than in the standard-care group in the first year after randomization and highlight the need for strict prevention measures and aggressive treatment of Covid-19 in patients receiving CAR-T therapies. After safety measures that were consistent with international guidelines were introduced, no deaths related to Covid-19 occurred in the cilta-cel group (see the Supplementary Appendix). The incidence of Covid-19 infection that was considered to have occurred during a trial treatment was lower in the cilta-cel group than in the standard-care group (13.9% vs. 26.4%). Furthermore, the incidence of all infections during the trial period was similar with cilta-cel and standard care (62.0% vs. 71.2%), which suggested that with appropriate prophylaxis and treatment, infection risk is generally treatable in patients receiving cilta-cel.
Overall, CAR-T–specific adverse events were manageable with appropriate supportive care. Lower rates of cytopenias, cytokine release syndrome, and CAR-T–related neurotoxicity were seen in CARTITUDE-4 than in CARTITUDE-1, which suggests that cilta-cel may have a better side-effect profile when used earlier in treatment.10,11 Effective bridging therapy enables better control of tumor burden before CAR-T infusion. The incidence of movement and neurocognitive adverse events was also lower in CARTITUDE-4 (0.6%) than in CARTITUDE-1 (6.0%),10,11 a difference that may be related to management strategies that were implemented to mitigate this risk.28 Cranial nerve palsies are a recognized side effect of CAR-T therapies,10,29 and such events that were observed in our trial were mild to moderate; most cases had resolved by the data-cutoff date. No clear risk factors for cranial nerve palsies have been identified, and the mechanism is not understood.
In this trial, we found a favorable risk–benefit profile for a single infusion of cilta-cel as compared with standard care. As with other myeloma treatments, real-world translation of clinical trial results will be influenced by a variety of factors, including patient selection and fitness, patient heterogeneity, treatment accessibility and setting, and patient or physician preference.30 Nonetheless, the strong progression-free survival benefit and rapid and deep response with cilta-cel highlight the potential for cilta-cel to become a therapeutic option for patients with myeloma after the first relapse.
Supported by Janssen Research and Development and Legend Biotech USA. Dr. Popat is supported by the Biomedical Research Centre, National Institute for Health and Care Research, University College London Hospitals.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
Drs. San-Miguel and Dhakal contributed equally to this article.
This article was published on June 5, 2023, at NEJM.org.
A data sharing statement provided by the authors is available with the full text of this article at NEJM.org.
We thank the patients who volunteered to participate in the trial, along with their families and caregivers; the physicians and nurses who cared for the patients and supported this clinical trial; the staff members at the 81 trial sites in the United States, Europe, Australia, and Asia who enrolled patients and staff members who were involved in data collection and analysis; John Fastenau and Katherine Gries for their assistance with data analysis; Tito Roccia and William Deraedt for their critical review of the manuscript; members of Venn Life Sciences for providing support for the data analysis; and Niraja Suresh, Sandi Wong, and Andrew Marson of Eloquent Scientific Solutions for medical writing support with an earlier version of the manuscript.
Author Affiliations
From the Cancer Center Clínica Universidad de Navarra, Centro Investigación Medica Aplicada, Instituto de Investigación de Navarra, Centro Investigación Biomédica en Red Cáncer (CIBERONC), Pamplona (J.S.-M.), the University Hospital of Salamanca, Instituto de Investigación Biomédica de Salamanca, Centro Investigación del Cáncer, CIBERONC, Salamanca (M.-V.M.), the Amyloidosis and Myeloma Unit, Department of Hematology, Hospital Clínic of Barcelona, Institut d’Investigacions Biomèdiques August Pi i Sunyer, University of Barcelona, Barcelona (C.F.L.), the Hematological Malignancies Clinical Research Unit, Hospital 12 de Octubre Universidad Complutense, Centro Nacional de Investigaciones Oncológicas, CIBERONC, Madrid (J.M.-L.), and the Institut Català d’Oncologia and Institut Josep Carreras, Hospital Germans Trias i Pujol, Badalona (A.O.) — all in Spain; the Medical College of Wisconsin, Milwaukee (B.D.); the University College London Cancer Institute (K.Y.) and University College London Hospitals, NHS Foundation Trust (R.P.), London, University Hospitals Bristol and Weston NHS Foundation Trust, Bristol (J. Griffin), and Janssen Research and Development, High Wycombe (J. Gilbert) — all in the United Kingdom; Monash University (A. Spencer) and the Peter MacCallum Cancer Centre and Royal Melbourne Hospital, Sir Peter MacCallum Department of Oncology, University of Melbourne (S.J.H.), Melbourne, VIC, and Royal Prince Alfred Hospital and the University of Sydney, Sydney (P.J.H.) — all in Australia; the Vaccine and Infectious Disease Institute, University of Antwerp, Antwerp, and the Division of Hematology and Center for Cell Therapy and Regenerative Medicine, Antwerp University Hospital, Edegem — both in Belgium (S.A.); the Department of Hematology, University Hospital Hôtel-Dieu, Nantes (P.M., C.T.), and Service d’Hématologie et Thérapie Cellulaire, Hôpital La Milétrie, and Centre d’investigation Clinique INSERM 1402, Poitiers University Hospital, Poitiers (X.L.) — both in France; Tel Aviv Sourasky Medical Center (I.A., Y.C.C.) and the Sackler Faculty of Medicine, Tel Aviv University (Y.C.C.) — both in Tel Aviv, Israel; IRCCS Azienda Ospedaliero–Universitaria di Bologna, Seràgnoli Institute of Hematology, and the Department of Medical and Surgical Sciences, Bologna University School of Medicine, Bologna, Italy (M.C.); the Department of Hematology, Japanese Red Cross Medical Center, Tokyo (T.I.); the Division of Hematology–Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea (S.J.K.); the Department of Hematology, University Medical Center Groningen, Groningen (W.R.), and Amsterdam University Medical Center, Vrije Universiteit Amsterdam, Amsterdam (N.W.C.J.D.) — both in the Netherlands; Poznan University of Medical Sciences, Poznan, Poland (D.D.); Stanford University School of Medicine, Stanford, CA (S.S.); the University of Alabama at Birmingham, Birmingham (L.J.C.); Ohio State University Comprehensive Cancer Center, Columbus (A.M.K.); Janssen Research and Development, Raritan (N.L., J.M.S., C.C.J., K.C., T.Y., S.N.), and Legend Biotech, Somerset (E.F., L.P., N.P.) — both in New Jersey; Janssen, Buenos Aires (C.L.); Cilag International, Zug, Switzerland (A. Slaughter); Janssen Research and Development, Spring House, PA (K.L., E.Z.); Janssen China Research and Development, Shanghai (D.C.); and Universitätsklinikum Würzburg, Medizinische Klinik und Poliklinik II, Würzburg, Germany (H.E.).
Dr. San-Miguel can be contacted at sanmiguel@unav.es or at Clínica Universidad de Navarra, Avenida Pio 12, 36 Pamplona 31008, Navarra, Spain.

