
Reference article: Heiss MW, Mancini R, Ayres C. Implementation of a Cardio-Oncology Pharmacist Position in a Community Cancer Center. J Hematol Oncol Pharm. 2026;16(2):1-7.
The field of cardio-oncology developed to meet the increased demand for care among patients with cancer who have pre-existing cardiovascular disease or who develop cardiotoxicity secondary to cancer treatment.1,2 With the growing list of oncolytic agents, the number of agents associated with newly identified cardiac adverse effects (AE) continues to increase.3 Pharmacists play a unique role in the multidisciplinary team.4 They are the medication experts who can provide education to patients and members of the care team, and help cardio-oncology teams stay up-to-date with our rapidly evolving field.1,4 They also have extensive knowledge of potential drug-drug interactions, AE profiles, and efficacy and safety of medications.1,4
The need to mitigate the knowledge gap between the oncology and cardiology fields provided an opportunity to implement an oncology pharmacist in an established cardio-oncology clinic. An oncology pharmacist proposed conducting a single-center, 4-week pilot rotation from February 5, 2024 to March 8, 2024 working as a cardio-oncology pharmacist at a community cancer center. The goals of this pilot were to define the role of the pharmacist in this setting, including types of documentation, to provide guideline-directed interventions, and to develop a framework for other institutions seeking to add an oncology pharmacist in this setting.
The project development phase included a literature search on the pharmacist’s role and meetings with pharmacists across the United States who have established cardio-oncology practices or have been key in the development of this role nationally. This crucial step led to important documentation examples and resources, including the 2022 European Society of Cardiology (ESC) Guidelines on cardio-oncology, articles from the Journal of the American College of Cardiology: Cardio-oncology, and examples of pharmacist interventions.5
During the project implementation phase, the oncology pharmacist participated in 10 cardio-oncology clinics. The pharmacist collected workload metrics using an Excel spreadsheet, capturing data such as the number of patients seen in clinic, documentation completed, types of interventions performed, patient demographics, patients’ capacity to proceed with cancer treatment, educational activities provided by the pharmacist, and time allocated to each task. On days without clinic, the pharmacist completed chart reviews. Due to the time-consuming nature of chart review, the process was re-evaluated to prioritize new patients on active treatment or planned treatment, hematopoietic stem cell transplant recipients, and childhood and adolescent cancer survivors. Pharmacist-specific documentation evolved throughout the pilot project with the goal of complementing cardiologist documentation and providing valuable information for the oncology care team on oncolytic agents’ specific cardiac toxicities, drug-drug interactions, baseline cardiovascular risk based on the patient’s medical history and chemotherapy regimen, and a proposed monitoring plan based on patient risk factors and the 2022 ESC guidelines.
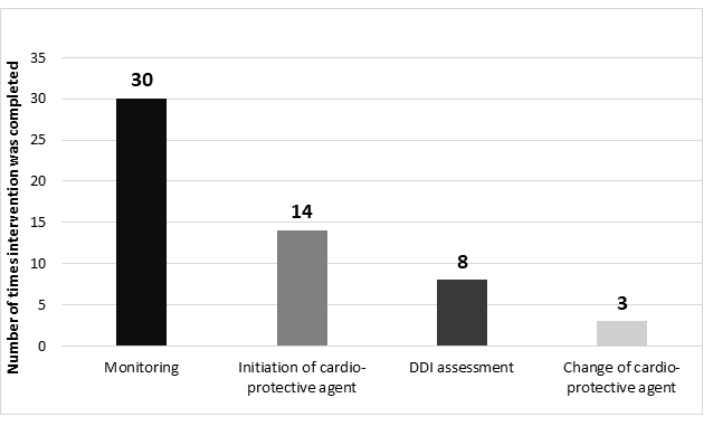
One hundred and eighteen patients were seen in the clinic, and fifty-seven patients were evaluated by the oncology pharmacist during this period. The average age of this population was 69 years. The most common cancer diagnoses were breast cancer, followed by diffuse large B-cell lymphoma and prostate cancer. A total of fifty-five interventions were completed by the pharmacist. Thirty-nine patients had at least one intervention and eight patients had two interventions completed per visit. The most common type of pharmacist intervention writing monitoring plans. These were based on guideline recommendations as well as the patient’s prior cardiovascular and cancer treatment history. Other pharmacist’s interventions consisted of initiation of cardioprotective therapy for the management of chemotherapy-induced cardiac AEs, assessment of drug–drug interactions, and changes in cardioprotective agents (Figure 1).
Figure 1. Types of Interventions/Recommendations (DDI = drug-drug interactions)
Pharmacist interventions occurred not only during cardio-oncology clinics, but also in other settings when patients experienced cardiac toxicity related to chemotherapy agents. One example was of a patient admitted to the hospital with suspected immune checkpoint inhibitor–induced myocarditis, for whom appropriate management and monitoring were recommended. Another example was of a patient with new-onset heart failure caused by lenvatinib, a vascular endothelial growth factor tyrosine kinase inhibitor, for whom recommendations on management, dose reduction, and appropriateness of medication re-trial were provided.
Despite the limited 4-week duration of this pilot project, the support and anticipated benefit of adding an oncology pharmacist to the cardio-oncology team led to the approval of a 0.5 full-time equivalent (FTE) position. Continued assessment of this role is needed to provide long-term data on pharmacist impact and overall clinical benefit in this patient population. Implementation of cardio-oncology-specific quality measures and a more accurate assessment of patient volumes to calculate a percentage of patients who would qualify for a cardio-oncology referral would be valuable metrics to help other institutions implement similar services. The role of the oncology pharmacist in this setting has continued to expand, including pharmacist-led follow-up visits under a collaborative practice agreement to manage blood pressure medications and titrate guideline-directed medical therapy.
The development of a cardiac acuity tool within the electronic medical record (EMR) would help optimize prioritization of chart review for cardio-oncology pharmacists and bring attention to other oncology pharmacists evaluating treatment plans for patients at higher cardiovascular risk based on their comorbidities. An oncology pharmacist can play an important role in assessing patients before, during, and after cancer treatment, regardless of practice setting. The seven classes of agents highlighted by the 2022 ESC guidelines on cardio-oncology, for which patients should undergo baseline cardiovascular toxicity risk stratification are anthracyclines, HER2-targeted therapies, vascular endothelial growth factor inhibitors, BCR-ABL tyrosine kinase inhibitors, multiple myeloma therapies, MEK inhibitors, and therapies targeting the BRAF gene.5
The addition of a cardio-oncology pharmacist at our institution has also aided other oncology pharmacists via the implementation of specific monitoring actions in the EMR oncology treatment plans. For example, adding baseline serial troponin I measurements on treatment days for patients at high risk of anthracycline-induced cardiac toxicity, or adding baseline electrocardiogram and troponin I assessments for treatment plans containing immune checkpoint inhibitors. The cardio-oncology pharmacist has also assisted in risk assessment and cardio-oncology referral of patients who might be at high risk for chemotherapy-induced cardiac toxicity.
The implementation of an oncology pharmacist within an established cardio-oncology clinic demonstrated meaningful clinical contributions even within a limited 4-week pilot period. The pharmacist assisted in optimizing monitoring plans in alignment with current cardio-oncology guidelines, and identified and managed drug–drug interactions and cardiotoxicities. Future evaluation of expanded responsibilities during follow-up visits, along with extended data collection of interventions, is needed to more accurately reflect patient volume, optimize workflow, and further justify the addition of an oncology pharmacist FTE in this setting. Oncology pharmacists play a critical role in recognizing patients who are at increased risk for chemotherapy-induced cardiovascular AE, especially those with underlying cardiovascular risk factors. For more details on the methodology and results of this pilot, please refer to the original article.
References
-
Merali A, Anwar M, Boyd JM, et al. Exploration of current pharmacy practice in cardio-oncology: experiences & perspectives. J Oncol Pharm Pract. 2023;29:1844-1852.
-
Parent S, Pituskin E, Paterson DI. The cardio-oncology program: a multidisciplinary approach to the care of cancer patients with cardiovascular disease. Can J Cardiol. 2016;32:847-851.
-
White RT, Sirek ME, Marrs JC. Oral oncolytics and cardiovascular risk management and monitoring. J Cardiovasc Pharmacol. 2023;82:266-280.
-
Einsfeld L, do Canto Olegário I, Fagundes ML. Intersecting care through specialized pharmacists: a case report of residency rotation focused on the new horizon of cardio-oncology. Curr Pharm Teach Learn. 2023;15:508-513.
-
Lyon AR, López-Fernández T, Couch LS, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43:4229-4361. Erratum in: Eur Heart J. 2023;44:1621.


