Authors
- Katelynn Granger, PharmD, BCOP, Clinical Pharmacy Specialist in Malignant Hematology at Medical University of South Carolina
- Matthew Warrick, PharmD, BCPS, BCOP, Clinical Pharmacy Specialist in Malignant Hematology and Blood Marrow Transplant at Medical University of South Carolina
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma (NHL) in adults and accounts for roughly one-third of cases.1 This aggressive malignancy is treated in the front-line setting with chemoimmunotherapy such as R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) or Pola-R-CHP (with polatuzumab vedotin), leading to cure in approximately two-thirds of patients.2,3 For the remaining population who experience relapsed or refractory (R/R) disease, historical standards of care were limited and based on autologous stem cell transplant (ASCT) eligibility.4 Patients ineligible for ASCT would commonly receive less intensive platinum-based chemoimmunotherapy regimens such as R-GemOx (rituximab, gemcitabine, and oxaliplatin). However, as demonstrated by the SCHOLAR-1 trial, outcomes remained poor, with a mere seven percent of patients achieving complete remission (CR) after conventional salvage therapies.5
The emergence of three chimeric antigen receptor (CAR) T-cell therapy agents including axicabtagene ciloleucel, lisocabtagene maraleucel, and tisagenlecleucel, represented a major breakthrough in R/R NHL. A flurry of recent Food and Drug Administration (FDA) approvals in the R/R setting has now placed CAR-T as the standard of care in the third line setting, as well as in patients with primary refractory disease or those who are unfit for ASCT.6-14 Though CAR T-cell therapies demonstrate marked improvements in survival outcomes and potential cure in up to 30% of R/R patients, their utilization is not suitable or feasible for all patients. Treatment-related toxicities such as cytokine release syndrome (CRS), immune-effector cell-associated neurotoxicity syndrome (ICANS), cytopenias, hypogammaglobulinemia, and infections can lead to significant morbidity and non-relapse mortality.15 Furthermore, constraints such as distance from CAR-T centers, requirement for apheresis, timeline for product manufacturing, and cost can prove barriers for patients in areas with low healthcare resources or those in need of urgent treatment.
An off-the-shelf alternative in patients with R/R NHL has more recently emerged in the form of bispecific antibodies (BsAbs). These agents provide similar immune-mediated effects to CAR-T by way of co-targeting tumor antigens CD3 and CD20 and endogenous immune effector cells to induce tumor death. Two bispecific antibodies, glofitamab and epcoritamab, are FDA-approved as monotherapies in the third line setting for R/R DLBCL based on favorable results in their respective studies.16,17 With overall response rates (ORR) of 53% and 63%, respectively, as well as median duration of response approaching or exceeding 12 months, these agents represented a much-needed novel tool in the armamentarium for R/R DLBCL. Yet, there may be room for further improvement still, as investigators have begun to explore the novel combination of BsAbs with traditional chemotherapy regimens like gemcitabine and oxaliplatin to continue to further improve outcomes.
STARGLO: Glofitamab with GemOx
The global, phase III, randomized STARGLO trial evaluated the efficacy and safety of glofitamab plus gemcitabine and oxaliplatin (Glofit-GemOx) versus rituximab plus gemcitabine and oxaliplatin (R-GemOx) in 274 patients with R/R DLBCL who had received at least one prior line of therapy and were ineligible for ASCT.18 Patients were randomly assigned in a 2:1 ratio to receive Glofit-GemOx or R-GemOx and further stratified based on the number of prior therapies (one, two or more) and whether they were refractory to their last treatment. ASCT ineligibility was defined as age > 70 years, end organ dysfunction, Eastern Cooperative Oncology Group (ECOG) performance status of 2 or higher, patient refusal for ASCT, or other investigator-assessed comorbidities. Patients with confirmed double or triple hit lymphoma were not eligible.
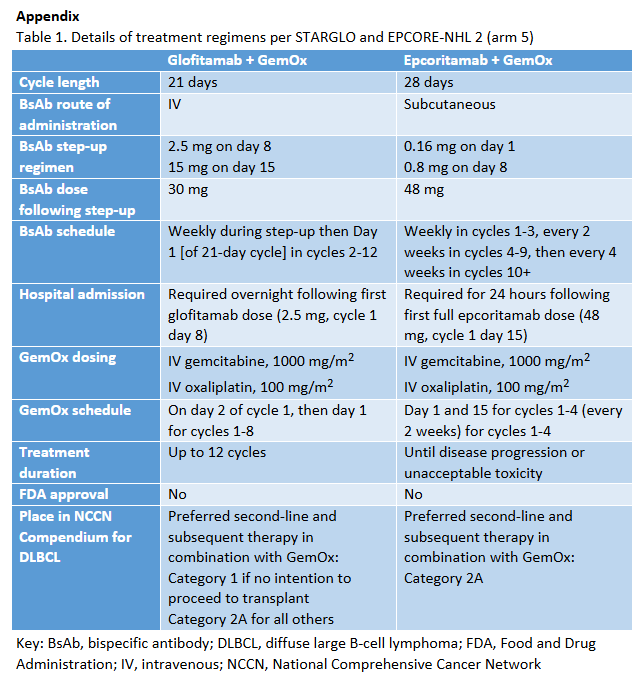
GemOx was administered using a 21-day dosing schema, given as gemcitabine 1000 mg/m2 and oxaliplatin 100 mg/m2 on day 2 of cycle 1 and then day 1 of the subsequent 7 cycles. In the control arm, rituximab 375 mg/m2 was given on day 1 of each cycle. To mitigate risk of CRS, patients in the study arm received pretreatment with obinutuzumab 1000 mg on cycle 1 day 1 before glofitamab was initiated. As demonstrated in Table 1, glofitamab was administered in weekly step-up doses of 2.5 mg on day 8 and 10 mg on day 15 of cycle 1, followed by fixed-dose 30 mg on day of cycles 2-12 in a similar strategy to the monotherapy indication. Granulocyte colony-stimulating factor was mandatory for all patients in cycles 1 and 2 for both arms.
Baseline characteristics were well-balanced between treatment groups, with nine percent of patients enrolled at study sites in the U.S. After a median follow-up of 20.7 months, the median investigator-assessed overall survival (OS) was 25.5 months (95% CI 18.3-NE) with Glofit-GemOx compared to 12.9 months (95% CI 7.9-18.5) with R-GemOx (HR = 0.62; 95% CI 0.43-0.88). Progression free survival (PFS) was also significantly longer in the Glofit-GemOx group, with a median independent review committee (IRC) PFS of 13.8 months (95% CI 8.7-20.5) compared to just 3.6 months (95% CI 2.5-7.1) with R-GemOx, resulting in over a 60% reduction in risk of disease progression or death (HR = 0.4, 95% CI 0.28-0.57). The use of glofitamab with GemOx also improved complete response (CR) rates more than twofold at 58.5% compared to 25.35% with R-GemOx.
A notable safety concern with BsAbs is the incidence of CRS and ICANs. In this study, CRS occurred in 76 (44%) of glofitamab-exposed patients, with 2% experiencing grade 3 symptoms. CRS occurred most commonly after the initial 2.5mg glofitamab dose, with a median onset of 13.6 hours. ICANS was reported in four (2%) of patients, with one (1%) developing a grade 3 event. All ICANS events were reported concurrently with CRS and resolved with CRS resolution. Rates of serious infections were higher in the Glofit-GemOx group, occurring in 26% of patients as compared to 13% in R-GemOx. Seven patients (4%) in Glofit-GemOx expired from a COVID-19-associated grade 5 adverse event, while this did not occur in the R-GemOx arm.
EPCORE NHL-2, Arm 5: Epcoritamab with GemOx
EPCORE NHL-2 was a phase 1b/2 open-label multinational trial investigating the use of epcoritamab with various other standard-of-care agents in patients with R/R CD20+ non-Hodgkin lymphoma. There were ten arms in total, assessing epcoritamab in combination with agents such as R-CHOP in newly diagnosed DLBCL and rituximab and lenalidomide in patients with newly diagnosed and, in a separate arm, R/R follicular lymphoma.
Arm 5 of EPCORE NHL-2 specifically examined the use of epcoritamab with GemOx (Epco-GemOx) in patients with R/R DLBCL who were ineligible for or had failed ASCT.19 Patients were required to have CD20+ DLBCL relapsed or refractory to at least 1 line of therapy, an ECOG score of 0-2, and either previous ASCT failure or ineligibility for ASCT due to age, performance status, or comorbidities. Patients were not excluded with double- or triple-hit lymphoma, nor for having previous CAR T-cell therapy.
Epcoritamab was given subcutaneously weekly in cycles 1-3, every 2 weeks in cycles 4-9, then every 4 weeks in cycles 10 and beyond until disease progression or unacceptable toxicity in a 28-day cycle. The first two doses were weekly step-up doses of 0.16 mg and 0.8 mg, followed by 48 mg as above. Gemcitabine and oxaliplatin were given IV every 2 weeks in cycles 1-4 (1000 mg/m2 and 100 mg/m2, respectively).
After a median follow-up of 13.2 months (range 1-34.6), ORR and CR rates were 85% and 61% by IRC assessment. Median PFS among patients overall and with a CR was 11.2 (95% CI, 8-14.7) and 26.7 (95% CI, 11.7- not reached [NR]) months. Median OS among patients overall and with a CR was 21.6 months (95% CI, 11.6-NR) and NR (95% CI, NR-NR), respectively. The median time to response was 1.5 months and median time to CR was 2.6 months. Subgroup analyses demonstrated better CR rates in patients with 1 prior line of therapy (pLOT) compared to ≥2 (74% vs 53%) and in patients who were CAR-T naïve (68% vs 45%). Of note, 3 patients with initial PRs converted to CR by 24 weeks and 3 patients with initial stable disease had a PR or CR by week 12, suggesting that responses may deepen with time.
The most common adverse events included hematologic adverse events such as thrombocytopenia (any grade, 75.8%; grade ≥3, 59.2%), neutropenia (any grade, 65%; grade ≥3, 57.3%), and anemia (any grade, 59.2%; grade ≥3, 42.7%. Infections were notable, arising in 71.8% of patients with grade ≥3 in 29.1%. CRS also occurred in 52.4% of patients with grade ≥3 CRS occurring in 1%. ICANS occurred in 2.9% of patients grade ≥3 ICANS occurring in 1%.
Discussion/Clinical Considerations
STARGLO and EPCORE NHL-2 are the first studies to examine the use of BsAbs in combination with chemotherapy in patients with R/R DLBCL. These trials validated the concept that use of Glofit-GemOx and Epco-GemOx, respectively, can lead to excellent response rates with durable remissions in patients with R/R DLBCL who are ineligible for ASCT. While neither regimen has received FDA approval at this time, the National Comprehensive Cancer Network (NCCN) has included the two regimens as preferred therapies in the second line setting for non-candidates for CAR-T or ASCT, with a category 1 recommendation for Glofit-GemOx in ASCT-ineligible patients.20
Despite this significant stamp of approval from NCCN, it is important to note that limitations still exist for each study. While Glofit-GemOx demonstrated improved outcomes as compared to R-GemOx,it must be conceded that R-GemOx is not considered an NCCN preferred second-line option in patients with R/R DLBCL who are not candidates for transplant. Therefore, in the current treatment landscape of novel immunotherapy combinations, the comparator arm may be considered substandard. Furthermore, by excluding patients with double- and triple-hit lymphoma, the STARGLO trial may limit generalizability to these notoriously difficult-to-treat populations. On the other hand, EPCORE NHL-2 results are limited by the lack of a comparator arm and therefore warrant further investigation.
Lastly, while both studies focus on the non-transplant-eligible population, the evolving role of ASCT - driven by the emergence of CAR T-cell therapy, particularly in the second line setting - raises important questions about how bispecific antibody regimens should be optimally sequenced among these alternative therapies.
Practical Considerations for Administration
Though their role of BsAb regimens in clinical practice continues to expand, considerable barriers still exist that may hinder smooth implementation in the real-world setting. Even with lower rates of severe CRS and ICANS compared to CAR-T, community practices less familiar with management of these unique toxicities, especially those who do not have the infrastructure to administer CAR T-cell therapy, may be hesitant to utilize BsAb regimens.
As outlined in Table 1, both BsAb regimens have unique considerations for administration. Patients receiving Glofit-GemOx, are required to receive pre-treatment with one dose of obinutuzumab prior to initiation to minimize risk of CRS. While Epco-GemOx does not require pretreatment with obinutuzumab, its schedule is more onerous and entails weekly epcoritamab injections for 12 weeks through cycle 3. The chemotherapy component of Glofit-GemOx is administered in 21-day cycles, as compared to Epco-GemOx, which employs a 14-day cadence. This more aggressive chemotherapy schedule, in addition to the increased frequency or epcoritamab injections, may be more challenging for patients to tolerate.
Coordinating BsAb step-up regimens alongside concomitant cytotoxic chemotherapy presents logistical challenges, particularly in managing overlapping toxicities such as infection risk and cytopenias. The complexity of adverse effect management increases with the use of multiple agents, requiring close monitoring and supportive care. Numerous publications have outlined tips and tricks for operationalizing bispecific antibodies across a variety of indications. Key recommendations include robust healthcare provider education, leveraging the electronic health record to streamline adverse event and supportive care management, and concerted coordination among oncology centers. 21-22
Conclusions
A novel area of investigation in R/R DLBCL is the combination of bispecific antibodies such as glofitamab and epcoritamab with chemotherapy in R/R DLBCL. Studies exploring this new treatment schema utilizing off-the-shelf immunotherapy agents have demonstrated better response rates and more durable remissions as compared to traditional chemoimmunotherapy. As a tolerable option in patients who are ineligible for ASCT, without the limitations that accompany CAR T-cell therapies, patients may have a new option in a difficult-to-treat disease state. Questions remain regarding optimal sequencing among CAR T-cell therapy and BsAb regimens. Real-world data will help provide additional insight into the efficacy and tolerability of these regimens.
References
1.Wang SS. Epidemiology and etiology of diffuse large B-cell lymphoma. Semin Hematol. 2023;60(5):255-266.
2.Coiffier B, Thieblemont C, Van Den Neste E, et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d'Etudes des Lymphomes de l'Adulte. Blood. 2010;116(12):2040-2045. doi:10.1182/blood-2010-03-276246
3.Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N Engl J Med. 2022;386(4):351-363. doi:10.1056/NEJMoa2115304
4.Gisselbrecht C, Glass B, Mounier N, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era [published correction appears in J Clin Oncol. 2012 May 20;30(15):1896]. J Clin Oncol. 2010;28(27):4184-4190.
5.Crump M, Neelapu SS, Farooq U, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study [published correction appears in Blood. 2018 Feb 1;131(5):587-588. Blood. 2017;130(16):1800-1808.
6.Neelapu SS, Locke FL, Bartlett NL, et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med. 2017;377(26):2531-2544.
7.Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med. 2019;380(1):45-56.
8.Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020;396(10254):839-852.
9.Neelapu SS, Jacobson CA, Ghobadi A, et al. Five-year follow-up of ZUMA-1 supports the curative potential of axicabtagene ciloleucel in refractory large B-cell lymphoma. Blood. 2023;141(19):2307-2315.
10.Locke FL, Miklos DB, Jacobson CA, et al. Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma. N Engl J Med. 2022;386(7):640-654.
11.Westin JR, Oluwole OO, Kersten MJ, et al. Survival with Axicabtagene Ciloleucel in Large B-Cell Lymphoma. N Engl J Med. 2023;389(2):148-157.
12.Bishop MR, Dickinson M, Purtill D, et al. Second-Line Tisagenlecleucel or Standard Care in Aggressive B-Cell Lymphoma. N Engl J Med. 2022;386(7):629-639.
13.Abramson JS, Solomon SR, Arnason J, et al. Lisocabtagene maraleucel as second-line therapy for large B-cell lymphoma: primary analysis of the phase 3 TRANSFORM study. Blood. 2023;141(14):1675-1684.
14.Sehgal A, Hoda D, Riedell PA, et al. Lisocabtagene maraleucel as second-line therapy in adults with relapsed or refractory large B-cell lymphoma who were not intended for haematopoietic stem cell transplantation (PILOT): an open-label, phase 2 study. Lancet Oncol. 2022;23(8):1066-1077.
15.Brudno JN, Kochenderfer JN. Current understanding and management of CAR T cell-associated toxicities. Nat Rev Clin Oncol. 2024;21(7):501-521.
16.Dickinson MJ, Carlo-Stella C, Morschhauser F, et al. Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N Engl J Med. 2022;387(24):2220-2231. doi:10.1056/NEJMoa2206913
17.Thieblemont C, Phillips T, Ghesquieres H, et al. Epcoritamab, a Novel, Subcutaneous CD3xCD20 Bispecific T-Cell-Engaging Antibody, in Relapsed or Refractory Large B-Cell Lymphoma: Dose Expansion in a Phase I/II Trial. J Clin Oncol. 2023;41(12):2238-2247. doi:10.1200/JCO.22.01725
18.Abramson JS, Ku M, Hertzberg M, et al. Glofitamab plus gemcitabine and oxaliplatin (GemOx) versus rituximab-GemOx for relapsed or refractory diffuse large B-cell lymphoma (STARGLO): a global phase 3, randomised, open-label trial. Lancet. 2024;404(10466):1940-1954. doi:10.1016/S0140-6736(24)01774-4
19.Brody JD, Jørgensen J, Belada D, et al. Epcoritamab plus GemOx in transplant-ineligible relapsed/refractory DLBCL: results from the EPCORE NHL-2 trial. Blood. 2025;145(15):1621-1631. doi:10.1182/blood.2024026830
20.NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): B-cell Lymphomas. Version 2.2025. Updated February 10, 2025. Accessed April 20, 2025.
21.Olivieri DJ, Banerjee R. Impatient for outpatient: operationalizing bispecific antibodies for multiple myeloma in the ambulatory setting. JCO Oncol Pract. Published online December 20, 2024:OP2400921.
22.Mahmoudjafari Z, Ali, A, Davis J, Sandahl T, Nachar V, Mancini, R. Seamless navigation of bispecific therapies: optimizing management and outpatient access with a focus on coordination. JADPRO. 2024;15(8).