Authors
- Aracely Sosa, PharmD, PGY1 Pharmacy Resident at University of Texas Southwestern Medical Center, Dallas, TX
- Katelyn Toeniskoetter, PharmD, BCOP, Disease Group Research Pharmacist, Thoracic at Dana Farber Cancer Institute, Boston, MA
- Pearl Abraham, PharmD, BCPS, BCOP, Clinical Pharmacy Specialist Transplant and Cellular Therapies at University of Texas Southwestern Medical Center, Dallas, TX
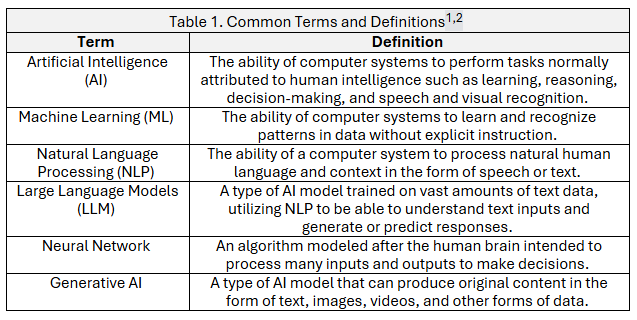
Artificial intelligence (AI) is transforming many industries, and medicine is no exception. Although AI has made significant strides in medicine and in pharmacy, the concept of AI can be a foreign concept for many pharmacists. Because the term “AI” encompasses a broad scope of different algorithms and models, it is important to differentiate the terminology used in this space. Having this basic understanding of AI can help pharmacists become familiar and comfortable with these concepts. The table below includes common terms and definitions that can be encountered in discussions regarding AI.1,2
While the use of AI in pharmacy is still limited, there have been several publications investigating the implementation of AI in oncology pharmacy.
Current use of AI in oncology pharmacy
Treatment decision making support
The role of LLMs in decision-making within a fast-changing area such as oncology has been studied for accuracy and efficiency. A study comparing the accuracy of information in oncology questions showed that OpenAI’s GPT-4 was superior to Meta’s LLaMA 1, Google’s Bard/PaLM 2, Anthropic’s Claude-v1, and OpenAI’s GPT-3.5, achieving the highest overall accuracy of 69%.3 Similarly, a retrospective study conducted at a French cancer center evaluated the clinical relevance and accuracy of several LLMs - specifically Claude3-Opus, GPT-4 Turbo, and LLaMa3-70B - in generating treatment recommendations for patients with early-stage breast cancer. These AI-generated suggestions were compared to expert decisions made during multidisciplinary team (MDT) meetings. Concordance was defined as alignment between LLM outputs and expert recommendations. In instances of divergence, LLM recommendations were deemed "acceptable" if they adhered to established guidelines from the National Comprehensive Cancer Network (NCCN) or the European Society for Medical Oncology (ESMO). Among the 112 anonymized cases assessed between January and April 2024, 75% to 86.6% of the LLM-generated treatment suggestions were classified as appropriate. Claude3-Opus and GPT-4 Turbo demonstrated slightly higher performance metrics compared to LLaMa3-70B. These findings underscore the potential of generalist LLMs to support clinical decision-making in oncology. Further optimization, particularly through integration with domain-specific medical literature and datasets, may enhance their reliability and clinical utility.4
Patient messages
In the advent of patients seeking care virtually in a post-pandemic era, the burden on patient portal messages can be relieved by the use of an NLP algorithm to automate message triage through intelligent routing. A study done at Emory showed that deploying an NLP algorithm to triage patient messages into 5 pre-set categories (urgent, clinician, refill, schedule, form) allowed for significantly shorter time to first message interaction (median 0.2 hours vs 1.2 hours), and quicker resolution of messages compared to the control group (median 4.2 hours vs 26.7 hours). This allows for enhanced operational efficiency within healthcare organizations, reduced administrative burden, and decreased burnout among healthcare workers.5 Likewise, LLMs can also be utilized to relieve clinician burden in submitting for prior authorizations and appeal letters.
Patient education
LLMs can be used to create patient education materials that help explain complex oncology treatment plans and the related supportive care. In one study, researchers compared the effectiveness and readability of AI-generated materials with those created by physicians for common side effects such as cytopenia, diarrhea/constipation, fatigue, nausea, neuropathy, and loss of appetite. The results showed that GPT-4 produced content of comparable quality to that written by physicians. While evaluators slightly preferred the physician-generated materials, the AI content was noted for being concise and well-organized.6 These findings suggest that tools like ChatGPT, especially when reviewed by healthcare professionals, can be valuable for developing accurate and accessible educational content in oncology.
Disease/drug monitoring
Clinical Decision Support Systems (CDSS), such as AI-enhanced platforms like IBM Watson for Oncology (WFO), provide real-time alerts and treatment recommendations based on evolving clinical guidelines, aiding pharmacists in optimizing chemotherapy regimens.7 Predictive analytics tools, trained on electronic health records and pharmacogenomic data, help forecast adverse events. Alfieri, et al. used a deep learning model, to predict AKI episodes more than 12 hours in advance in an ICU setting.8
One recent study demonstrated the utility of AI in predicting survival outcomes for renal cell carcinoma (RCC) patients receiving targeted therapy using radiomics and CT imaging data. By extracting tumor features through the UPerNet algorithm and employing machine learning models, the researchers developed a highly accurate predictive tool, achieving over 93% accuracy in classifying patients into long- or short-survival groups.9 This kind of modeling can support pharmacists in identifying patients who may benefit from closer therapeutic monitoring or adjusted drug regimens. For instance, pharmacists could prioritize high-risk patients for more intensive follow-up or recommend changes in therapy based on survival probabilities derived from AI models.
Furthermore, ML and deep learning models have enabled real-time disease progression tracking by analyzing tumor imaging and laboratory data, which supports adjusting or discontinuing treatment plans proactively. For example, predictive models have been developed for predicting cardiotoxicity in breast cancer patients on anthracycline based therapy.10 NLP algorithms are being deployed to mine unstructured patient notes and records for early detection of underreported side effects, thereby improving pharmacovigilance.9 These and similar tools enable early identification of at-risk patients, supporting providers in making personalized treatment adjustments and enhancing cardiac safety in oncology care.
Pharmacy operations
From predictive inventory management to automated auditing and regulatory compliance tracking, the pharmacy sector presents a dynamic and fertile landscape for AI-driven transformation. Leveraging real-time demand data, localized health trends, and historical utilization patterns, pharmacies can employ AI to optimize inventory systems, including the automation of supply reordering processes to reduce waste and prevent stockouts. Moreover, AI technologies can alleviate the burden of routine tasks such as medication dispensation and logistical management, thereby enabling pharmacy professionals to redirect their focus toward more complex, patient-centered care activities that demand clinical expertise and human judgment.11
Clinical trials
AI is playing an increasingly vital role in transforming clinical trials, particularly in oncology, where rapid data analysis and patient-specific insights are essential. AI is being used to improve the efficiency of clinical trial design by analyzing prior studies, real-world data, and patient registries to simulate outcomes and refine inclusion criteria. For instance, traditional trials, which focused on tumor location and histology, are being replaced by innovative designs that prioritize genetic and molecular characteristics of tumors.12 ML models are also being applied to improve patient recruitment by matching eligible candidates to trials through automated analysis of electronic health records (EHRs) and genetic data. A system called MatchMiner–AI matches patients to potential trials based on core criteria, like tumor genomics.13 Systems such as this not only reduce administrative burden but can ensure enrollment of more diverse and representative populations.14
AI supports drug development and repurposing efforts by simulating pharmacodynamics and pharmacokinetics of novel compounds or repositioned drugs. An AI tool called XGDP that helps predict how cancer drugs will work in different patients by looking at both the drug's structure and the patient's gene activity. Unlike many AI models that act like black boxes, this one also explains why a drug might or might not work by highlighting key chemical features and gene interactions. This means AI can not only suggest which drugs might be most effective for specific patients but also provide insights into how the drugs work - which allows more confident treatment decisions early on in development.15
Academia
As AI becomes increasingly integrated into pharmacy practice, there is a growing imperative for pharmacy educators to adapt curricula to reflect its evolving role. AI tools offer students a range of applications, including the creation of customized study aids, the organization of both oral and written presentations, and the development of patient education resources, among others. Educators and pharmacist preceptors play a critical role in guiding students to refine their interactions with these technologies particularly in crafting precise and thoughtful prompts to ensure that outputs are both accurate and clinically relevant.
While some may express concern that the incorporation of AI into educational settings could impede the development of independent critical thinking skills, such risks can be effectively mitigated. Through deliberate instructional strategies and by modeling appropriate, evidence-based use of AI, educators can underscore the importance of discernment and professional judgment in conjunction with technological assistance.16,17
Challenges and implications of AI in pharmacy
Although AI utilization in pharmacy practice has demonstrated possible benefits, there remain questions about the challenges of using AI and the implications of incorporating AI into practice.
Bias
AI presents several complex challenges that are important to consider within the medical field. One such challenge is that of bias, or the inclination of AI to present certain data or recommend certain therapies without being inclusive of all available data. This is not necessarily the fault of the AI model, but rather the humans who have trained the model. The model itself can only utilize data that it has been trained on, and the data must be adequately accessible to the model. Therefore, if there is additional data and resources that it cannot access or wasn't taught, it cannot provide recommendations that are inclusive of that data. One way to address this issue is to train AI models on massive datasets that are all-encompassing and diverse to limit the inherent bias that may occur with smaller training datasets. Unfortunately, it is important to realize that AI remains a man-made machine, and unintentional biases may be inherited into the model via the training provided by humans.18
Generalizability
AI models are being created and trained in many institutions, both nationally and internationally. While these models have shown promise to be beneficial systems within pharmacy practice, one consideration to keep in mind is the generalizability of their model to one’s own institution. Workflows, technologies, regulations, and patient populations may differ between those demonstrated in studies to those at other institutions. This can make implementation of AI difficult as there is often no “one-size-fits-all" AI model that can be integrated into any kind of health system, and it may be hard to know whether the benefits of a particular AI model at one institution would be seen at others.18
Credibility
Generative AI models, such as OpenAI’s ChatGPT or Google’s Gemini, have massive potential in the healthcare field. The massive datasets with which they are trained provide substantial information for these models to be able to potentially generate appropriate recommendations to posed clinical questions. However, there have been issues reported with generative AI models and the credibility of recommendations provided. One issue is the lack of supporting sources for the recommendations the model is making. These models often do not reveal what information they used to come up with their response. Another concern is a phenomenon called “AI hallucinations” that have occurred with generative AI models. In these instances, the model generates fabricated or baseless responses. These inaccurate or incomplete outputs can lead to mistrust of the AI model, thus limiting its potential in a healthcare setting.18,19
Other implications
The Healthcare Portability and Accountability Act (HIPAA) of 1996 was created with the purpose of protecting patient health information. When HIPAA was enacted, there was no knowing where the advent of advanced healthcare technology would end up today - with AI-enabled machines. As mentioned before, AI models require training with data in order to learn then function as an intelligent machine. There comes a concern of data privacy and deidentification of health information when training these models with health-based data. It can be difficult to discern if the data being fed to the models has been appropriately managed to protect patient information. Federal regulations, while seemingly broad enough to afford patient privacy protection, have not directly addressed how to appropriately use AI in healthcare to ensure HIPAA standards have been met. There is ongoing discussion at the state level about implementing legislation that would create guardrails for AI and outline the responsible use of these systems in healthcare.20,21
AI has performed feats that could significantly impact pharmacy practice, such as treatment decision making, patient interaction, and operations. However, a point of contention for pharmacists with implementing AI in practice is the fear that AI will soon eliminate the need for pharmacists. 22 A crucial factor to consider is the distinct expertise of pharmacists in fostering meaningful relationships with both patients and healthcare providers, delivering tailored education, addressing barriers to healthcare access, critically evaluating complex clinical decisions, and navigating the nuanced aspects of clinical practice. These are competencies that, at present, remain beyond the capabilities of AI. 23 Instead, AI should be leveraged as a tool to streamline workflow, minimize errors, and automate administrative tasks to optimize pharmacists’ role in patient care.
Citations
1.Smoke S. Artificial intelligence in pharmacy: A guide for clinicians. American Journal of Health-System Pharmacy. 2024;81(14):641-646. doi:10.1093/ajhp/zxae051
2.Raza MA, Aziz S, Noreen M, et al. Artificial Intelligence (AI) in Pharmacy: An Overview of Innovations. Innov Pharm. 2022;13(2)doi:10.24926/iip.v13i2.4839
3.Rydzewski NR, Dinakaran D, Zhao SG, et al. Comparative Evaluation of LLMs in Clinical Oncology. NEJM AI. 2024;1(5):AIoa2300151. doi:doi:10.1056/AIoa2300151
4.Ah-thiane L, Heudel P-E, Campone M, et al. Large Language Models as Decision-Making Tools in Oncology: Comparing Artificial Intelligence Suggestions and Expert Recommendations. JCO Clinical Cancer Informatics. 2025;(9):e2400230. doi:10.1200/cci-24-00230
5.Anderson BJ, Haq MZu, Zhu Y, et al. Development and Evaluation of a Model to Manage Patient Portal Messages. NEJM AI. 2025;2(3):AIoa2400354. doi:doi:10.1056/AIoa2400354
6.Hui G, Jiang J, Dommaraju S, et al. Artificial intelligence vs. physicians: Quality of oncology patient education materials. JCO Oncology Practice. 2024;20(10_suppl):408-408. doi:10.1200/OP.2024.20.10_suppl.408
7.Jie Z, Zhiying Z, Li L. A meta-analysis of Watson for Oncology in clinical application. Scientific Reports. 2021/03/11 2021;11(1):5792. doi:10.1038/s41598-021-84973-5
8.Alfieri F, Ancona A, Tripepi G, et al. A deep-learning model to continuously predict severe acute kidney injury based on urine output changes in critically ill patients. J Nephrol. Dec 2021;34(6):1875-1886. doi:10.1007/s40620-021-01046-6
9.Ye J, Woods D, Jordan N, Starren J. The role of artificial intelligence for the application of integrating electronic health records and patient-generated data in clinical decision support. AMIA Jt Summits Transl Sci Proc. 2024;2024:459-467.
10.Chang W-T, Liu C-F, Feng Y-H, et al. An artificial intelligence approach for predicting cardiotoxicity in breast cancer patients receiving anthracycline. Archives of Toxicology. 2022/10/01 2022;96(10):2731-2737. doi:10.1007/s00204-022-03341-y
11.Al Meslamani AZ. Applications of AI in pharmacy practice: a look at hospital and community settings. J Med Econ. Jan-Dec 2023;26(1):1081-1084. doi:10.1080/13696998.2023.2249758
12.Fountzilas E, Tsimberidou AM, Vo HH, Kurzrock R. Clinical trial design in the era of precision medicine. Genome Medicine. 2022/08/31 2022;14(1):101. doi:10.1186/s13073-022-01102-1
13.Kehl KL, Mazor T, Trukhanov P, et al. Identifying Oncology Clinical Trial Candidates Using Artificial Intelligence Predictions of Treatment Change: A Pilot Implementation Study. JCO Precision Oncology. 2024;(8):e2300507. doi:10.1200/po.23.00507
14.Ismail A, Al-Zoubi T, El Naqa I, Saeed H. The role of artificial intelligence in hastening time to recruitment in clinical trials. BJR Open. 2023;5(1):20220023. doi:10.1259/bjro.20220023
15.Wang C, Kumar GA, Rajapakse JC. Drug discovery and mechanism prediction with explainable graph neural networks. Scientific Reports. 2025/01/02 2025;15(1):179. doi:10.1038/s41598-024-83090-3
16.Mortlock R, Lucas C. Generative artificial intelligence (Gen-AI) in pharmacy education: Utilization and implications for academic integrity: A scoping review. Explor Res Clin Soc Pharm. Sep 2024;15:100481. doi:10.1016/j.rcsop.2024.100481
17.Cain J, Malcom DR, Aungst TD. The Role of Artificial Intelligence in the Future of Pharmacy Education. American Journal of Pharmaceutical Education. 2023;87(10)doi:10.1016/j.ajpe.2023.100135
18.Labkoff S, Oladimeji B, Kannry J, et al. Toward a responsible future: recommendations for AI-enabled clinical decision support. J Am Med Inform Assoc. Nov 1 2024;31(11):2730-2739. doi:10.1093/jamia/ocae209
19.Hatem R, Simmons B, Thornton JE. A Call to Address AI "Hallucinations" and How Healthcare Professionals Can Mitigate Their Risks. Cureus. Sep 2023;15(9):e44720. doi:10.7759/cureus.44720
20.Rezaeikhonakdar D. AI Chatbots and Challenges of HIPAA Compliance for AI Developers and Vendors. J Law Med Ethics. 2023;51(4):988-995. doi:10.1017/jme.2024.15
21.Artificial Intelligence & Health Care: A Primer. August 20, 2024. Accessed April 15, 2025. https://www.ncsl.org/health/artificial-intelligence-health-care-a-primer
22.Hasan HE, Jaber D, Khabour OF, Alzoubi KH. Ethical considerations and concerns in the implementation of AI in pharmacy practice: a cross-sectional study. BMC Med Ethics. May 16 2024;25(1):55. doi:10.1186/s12910-024-01062-8
23.Siwicki B. Why AI will never eliminate the need for pharmacists. HIMSS Media; 2023. May 12, 2023, Accessed April 15, 2025. https://www.healthcareitnews.com/news/why-ai-will-never-eliminate-need-pharmacists