
What is the potential role for remestemcel-L-rknd in the treatment of steroid-refractory acute graft versus host disease?
- This therapy works by using the immunomodulatory effects of mesenchymal stromal cells (MSCs). MSCs inhibit T-cell activation, stopping T-cell proliferation and secretion of cytokines. In acute graft versus host disease (aGVHD), donor T-cells mount an immune response against the recipient through proliferation and cytokine release. These T-cells have a role in mediating systemic inflammation, cytotoxicity, and potential end organ damage.1, 2
- This product was approved in other countries, like Canada and New Zealand, before being approved in the United States (US). It was indicated for treatment in adults in these countries before being bought by its current owner and studied in pediatric patients. 2,3
- When studied under the original brand name of Prochymal®, as compared to placebo in the US study, remestemcel-L-rknd failed to meet its primary endpoint of durable complete response of steroid-refractory aGVHD (SR-aGVHD) lasting 28 days.
- Phase II European studies showed positive results of this product for orphan drug approval in the European Union.
- How the product was produced varied between the European and US studies, including donor source, culture methods and expansion levels, with the US product having larger scale proliferation of original donor sample compared to European proliferative expansion process.3
- The US study completed a subset analysis and had promising data for its use in pediatric patients.2,4
- Remestemcel-L-rknd, is the first Food and Drug Administration (FDA)-approved mesenchymal stromal cell therapy indicated for pediatric patients (≥ 2 months of age) who have SR-aGVHD. Steroids remain the first line therapy for aGVHD.1,5
- Other medications used in the second line setting for SR-aGVHD in pediatric patients include ruxolitinib, mycophenolate mofetil, anti-tumor necrosis factor (TNF) antibodies, extracorporeal photopheresis (ECP), and anti-thymocyte globulin (ATG).
- Patient-specific factors and institutional preferences contribute to treatment selection in SR-aGVHD.7
- Remestemcel-L-rknd was studied in MSB-GVHD001, a phase III, single arm study that enrolled 54 pediatric patients (2 months to 17 years of age) who failed to respond to systemic steroids in the first line setting for aGVHD post allogeneic hematopoietic cell transplant.
- Patients included had steroid refractory grade B to D aGVHD and excluded skin only grade B (based on the International Blood and Marrow Transplantation Registry Severity Index Criteria).
- Primary endpoint was overall response rate (ORR) at Day 28 from starting remestemcel-L-rknd compared to a pre-specified control value of 45%.
- ORR was achieved by 38 of 54 patients (70.4%) and was statistically superior to the derived control overall response (p = 0.0003).
- Overall survival was 74% through Day 100 and 98.5% through Day 180 from start of therapy.5
- Ruxolitinib was studied in the REACH 2 trial, a phase II trial that evaluated the use of ruxolitinib in 71 patients ages 12 and older, and in a single center retrospective study of patients ages 1 year of age and older. 9, 10, 11
- In the REACH 2 trial, day 28 ORR was 54.9%, including 26.8% of patient achieving a CR.10
- For the single center study, 11 patients were evaluated for response and five patients had a response by day 28.11
- Infliximab was studied in a multicenter retrospective chart review including 24 patients ages 3 months to 18 years of age. This study had an ORR of 82% for day 56 outcomes as defined by the study, but had a high level of graft versus host disease (GVHD) recurrence when therapy was discontinued.9,12
- Methotrexate used at low dose, of 10 mg/m2 weekly, was studied among 35 patients, ages 0 to 18 years, with 37% of patients achieving a CR for day 28 outcomes.9, 13
- There were 16 adverse events related to treatment in 9 patients
- Ten events were non-serious and included neutropenia, thrombocytopenia, cytomegalovirus infection, nausea, vomiting, pyrexia, allergic transfusion reaction, and hypotension.
- Six events were serious and included skin GVHD, adenovirus infection, Brookfield Kidney (BK) virus infection, hemolytic uremic syndrome, hypermetabolism, and somnolence.
- There were 14 deaths reported during the trial, and none were related to treatment with remestemcel-L-rknd. Most common reasons for death were disease relapse, aGVHD progression, infection, multiorgan failure, pulmonary hemorrhage, and cardiac arrest.5
What role can the pharmacist play in the management of patients on remestemcel-L-rknd?
- Administered as an infusion of 2 x106 MSC/kg body weight twice weekly for four weeks. Infusions should be administered at least three days apart.
- Patients should be premedicated with corticosteroids and antihistamines 30-60 minutes prior to infusion to reduce potential for infusion reactions.
- Administration rate
- For patients weighing ≥ 35 kg, remestemcel-L-rknd should be administered at a maximum rate of 6 mL/min.
- For patients weighing < 35 kg, remestemcel-L-rknd should be infused over 60 minutes.
- There are no renal or hepatic dose adjustments and no known drug interactions for this therapy.8
- Patients can continue steroids until eligible for steroid taper based on SR-aGVHD response and should remain on appropriate prophylactic anti-infective medications.5
- This medication should not be used in patients with known allergies to dimethyl sulfoxide (DMSO) or porcine and bovine proteins.
- This product is derived from the bone marrow of healthy human donors.
- There is a risk of transmission of infection from this product. This product contains cells from human donors and is manufactured using human, porcine, and bovine-derived reagents. The cell banks, reagents, and donors are screened for transmittable diseases, but they do not eliminate the risk of transmission of disease or agents.8
- Infections were the most common treatment emergent adverse effect, with serious infections including BK virus infection, staphylococcal infection, Epstein-Barr viremia, pneumonia, and sepsis. Two infections in the clinical trial were treatment related – adenovirus and BK virus infection.5
- Monitor for signs and symptoms of infections.
- Monitor for hypersensitivity reactions during infusion.
- Recommendations on repeat administration or discontinuation of treatment are based on 28-day response (Table 1).8
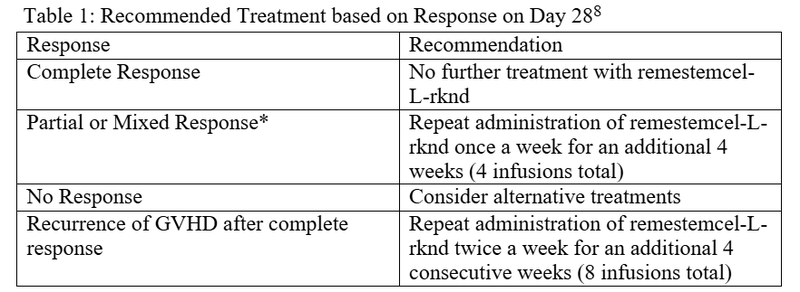
*Partial response for the trial was defined as organ improvement of at least one stage without worsening in any other organ. Mixed response was defined as improvement in at least one evaluable organ with worsening in another organ as per International Blood and Marrow Transplantation Registry Severity Index Criteria grading system.
Clinical Pearls
- Shipped directly to facility and must be frozen at ≤ -135 °C until thawed immediately prior to use.
- Infusion must occur within 5 hours of thawing therapy.
- Therapy is added to empty infusion bag along with plasma-lyte A.
- Single use vials. Dispose of empty or partially used vials per institutional guidelines for disposal of biohazardous materials.
- Ectopic tissue formation can occur as human mesenchymal cells can differentiate into mesenchymal lineage cells including bone, cartilage and fate cells.
- There is currently no patient assistance program.8
References
1.US Food and Drug Administration. FDA Approves First Mesenchymal Stromal Cell Therapy to Treat Steroid-refractory Acute Graft-versus-host Disease.
2.Wu, X., Jiang, J., Gu, Z. et al. Mesenchymal stromal cell therapies: immunomodulatory properties and clinical progress. Stem Cell Res Ther 11, 345 (2020). https://doi.org/10.1186/s13287-020-01855-9
3.Galipeau J. The mesenchymal stromal cells dilemma- does a negative phase III trial of random donor mesenchymal stromal cells in steroid-resistant graft-versus-host disease represent a death knell or a bump in the road?. Cytotherapy, 2013;15(1):2-8.
4.Antin JH. Steroid-Refractory Acute Graft-versus-Host Disease: Is There an Effective Therapy? Biol Blood Marrow Transplant. 2014 20: 145-148.
5.Kurtzberg J, Abdel-Azim H, Carpenter P, et al. A Phase 3, Single-Arm, Prospective Study of Remestemcel-L, Ex Vivo Culture-Expanded Adult Human Mesenchymal Stromal Cells for the Treatment of Pediatric Patients Who Failed to Respond to Steroid Treatment for Acute Graft-versus-Host Disease. Biol Blood Marrow Transplant. 2020;26(5):845-854. doi:10.1016/j.bbmt.2020.01.018
6.Lawitschka A, Lucchini G, Strahm B, et al. Pediatric acute graft-versus-host disease prophylaxis and treatment: surveyed real-life approach reveals dissimilarities compared to published recommendations. Transpl Int. 2020;33(7):762-772. doi:10.1111/tri.13601
7.Dignan FL, Clark A, Amrolia P, et al. Diagnosis and management of acute graft-versus-host disease. Br J Haematol. 2012;158(1):30-45. doi:10.1111/j.1365-2141.2012.09129.x
8.Ryoncil [Package Insert]. Mesoblast. New York, New York. 2024.
9.Gottardi F, et al. Treatment of steroid refractory graft versus host disease in children. Frontiers Transplant. 2023. 2. https://doi.org/10.3389/frtra.2023.1251112
10.Jagasia M, Perales MA, Schroeder MA, et al. Ruxolitinib for the treatment of steroid-refractory acute GVHD (REACH1): a multicenter, open-label phase 2 trial. Blood. 2020;135(20):1739-1749. doi:10.1182/blood.2020004823
11.Khandelwal P, Teusink-Cross A, Davies SM, et al. Ruxolitinib as Salvage Therapy in Steroid-Refractory Acute Graft-versus-Host Disease in Pediatric Hematopoietic Stem Cell Transplant Patients. Biol Blood Marrow Transplant. 2017;23(7):1122-1127. doi:10.1016/j.bbmt.2017.03.029
12.Sleight BS, Chan KW, Braun TM, Serrano A, Gilman AL. Infliximab for GVHD therapy in children. Bone Marrow Transplant. 2007;40(5):473-480. doi:10.1038/sj.bmt.1705761
13.Inagaki J, Fukano R, Kodama Y, Nishimura M, Shimokawa M, Okamura J. Safety and efficacy of low-dose methotrexate for pediatric patients with steroid-refractory acute graft-versus-host disease after hematopoietic stem cell transplantation. Ann Hematol. 2014;93(4):645-651. doi:10.1007/s00277-013-1923-x



