What is the potential role for obecabtagene autoleucel (obe-cel) in the treatment of relapsed refractory (r/r) B-cell acute lymphoblastic leukemia (B-ALL)?
- B-cell acute lymphoblastic leukemia is an aggressive hematologic malignancy involving abnormal lymphocyte proliferation resulting in presence of lymphoblasts. B-ALL is most common in the extremes of age with presence of Philadelphia chromosome as a key prognostic factor.
- Obe-cel is a CD-19 directed chimeric antigen receptor T-cell (CAR-T) agent with a 4-1BB co-stimulatory domain that enhances CAR-T proliferation and anti-tumor effect, while reducing risk of severe adverse effects, including cytokine release syndrome (CRS).¹
- Obe-cel was FDA-approved based on supporting evidence from the phase 1 ALLCAR19 and phase 1b/2 FELIX trials. ²⁻³
- The phase 1b/2 FELIX trial studied safety, efficacy, and scalability of obe-cel in adults with r/r B-ALL (n = 127).
- Baseline characteristics: previously treated with median 2 prior lines of therapy, majority received blinatumomab and/or inotuzumab ozogamicin and had a median of 40% bone marrow blasts. A total of 92.9% of patients required bridging therapy prior to receiving obe-cel.
- 120 patients received both doses of obe-cel. 7 patients only received 1 dose due to immunotoxic effects (n = 3), death due to cerebrovascular incident (n = 1), manufacturer related issue (n = 1), and rapid disease progression (n = 2).
- At median 21.5 months follow-up, among patients who received at least one dose of obe-cel:
- Primary endpoint in cohort 2A, who had ³ 5% bone marrow blasts at enrollment, defined as complete remission (CR) or complete remission with incomplete hematologic recovery (CRi) was met with 77% of patients in CR and 21% in CRi.
- Median event free survival was 11.9 months
- Estimated median overall survival was 15.6 months
- Median duration of response was 21.2 months²⁻⁴
- Other CAR-T therapy agents approved for r/r B-ALL in adults include tisagenlecleucel (tisa-cel) and brexucabtagene autoleucel (brexu-cel).
- Tisa-cel, brexu-cel, and obe-cel do not require hospital admission for post-infusion CRS and ICANS monitoring.
- For r/r B-ALL treatment, tisa-cel is currently only FDA-approved for patients up to 25 years of age.
- Head-to-head trials comparing safety and efficacy of CAR-T therapy agents are not currently available.
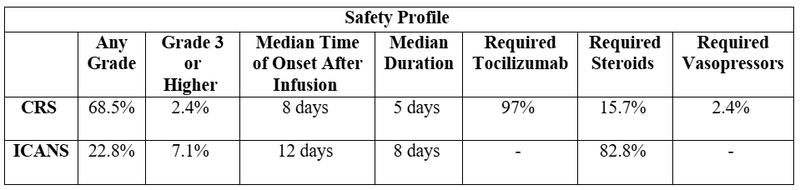
- However, overall response rates for all CAR-T therapy agents approximately fall within 70-80% with follow-up periods of 12-27 months. Safety concerns for CAR-T therapy in ALL treatment include CRS and ICANS. Lower incidences of grade 3 or higher CRS and ICANS have been observed with tisa-cel and obe-cel.⁵⁻⁶
What role can the pharmacist play in the management of patients on obe-cel?
- Provide education to patients and caregivers, highlighting safety concerns, such as CRS, ICANS, infections, key signs and symptoms to monitor for, and when to seek help.
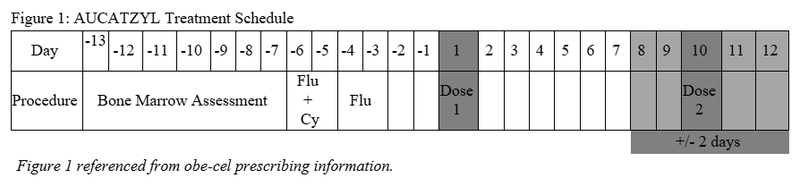
- Obe-cel administration is split over 2 days: days 1 and 10.
- After the first infusion, the manufacturer recommends monitoring at a healthcare facility for at least 7 days following each infusion, and for patients to remain within proximity of a healthcare facility for at least 2 weeks after each obe-cel infusion.
- Considering the risk of ICANS, the manufacturer recommends refraining from driving, hazardous occupations or activities, such as operating heavy or potentially dangerous machinery for 2 weeks following each obe-cel infusion.
- Following each infusion, patients and caregivers should continue to monitor signs and symptoms of CRS and ICANS for at least 2 weeks, such as level of consciousness, weakness, confusion, seizures, headaches, dizziness, fevers, and shortness of breath.¹
- Ensure appropriate supportive medications are ordered to mitigate risks of infection, seizure, and infusion reactions.
- Infection prophylaxis:
- Pneumocystis jiroveci pneumonia (PJP) and herpes simplex virus (HSV)/varicella zoster virus (VZV) prophylaxes are recommended with use of other CD19-targeting CAR-T therapy agents. Antibacterial and antifungal prophylaxis may be considered while a patient is neutropenic.
- Trend immune recovery after lymphodepletion and assess the need for antibacterial, antiviral, or antifungal prophylaxis.
- Hypogammaglobulinemia may occur, though guidelines currently do not address an optimal IgG monitoring frequency.
- IVIG 400-500 mg/kg monthly may be considered for serum IgG levels less than 400-600 mg/dL and if patient has serious or recurrent infections. IgG threshold for immunoglobulin replacement and immunoglobulin dosing are based on expert opinion and institutional practice.⁷⁻¹⁰
- Seizure prophylaxis:
- Seizure prophylaxis with levetiracetam 500-750 mg orally every 12 hours for 30 days starting the day of CAR-T infusion may be considered based on seizure risk.⁷ ¹¹
- Recommended pre-medication: acetaminophen approximately 30 minutes prior to obe-cel infusion.
- Corticosteroids should be avoided as a pre-medication due to concern for interference with efficacy of obe-cel.
- Infection prophylaxis:
- Ensure the correct lymphodepleting chemotherapy is selected for obe-cel with appropriate washout periods.
- Ensure patients are aware of expected timeline and side effects of lymphodepletion regimen.
- Recommended lymphodepleting chemotherapy regimen:
- Fludarabine 30 mg/m2/day IV days -6 to -3
- Cyclophosphamide 500 mg/m2/day IV days -6 to -5
- Obe-cel should be infused 3 days following completion of lymphodepleting chemotherapy, with a minimum 48 hour wash out period (may be delayed up to 4 days).
- In the months prior to initiating CAR-T therapy, pharmacists can help prepare patients by reviewing immunization history and screening for viral infections such as Human Immunodeficiency Virus (HIV), Hepatitis B Virus (HBV), Hepatitis C Virus (HCV), and possibly cytomegalovirus (CMV) infections.
- Pharmacists can support patients in obtaining updated vaccines in a timely manner with respect to CAR-T therapy timeline.
- Pharmacists can also facilitate management of HIV, HBV, HCV, CMV serologies, whether it be initiating treatment or prophylaxis.
- The safety of live vaccines has not been studied during or following obe-cel so live viral vaccines are not recommended for at least 6 weeks prior to the start of lymphodepleting chemotherapy treatment, during obe-cel treatment, and until subsequent immune recovery.
- Because obe-cel does not have a REMS program requiring tocilizumab to be stored on hand for each patient, the pharmacist can ensure tocilizumab is available.
Clinical Pearls
- Unlike other CAR-T products that split a single dose into multiple bags and administer them on the same day (e.g., lisocabtagene maraleucel), obe-cel is given as two separate doses on different days—specifically on Day 1 and Day 10.
- Obe-cel is supplied in infusion bags in metal cassettes via vapor phase liquid nitrogen shipper and should be transported to an on-site vapor phase liquid nitrogen storage with temperature at -150°C until product is ready to be thawed for administration. Time outside of liquid nitrogen should be minimized and is not recommended to exceed 90 seconds.
- Thaw obe-cel in its overwrap in a 37°C water bath or dry thaw method. Gently massage bag until thawed with no visible frozen clumps. Thawing typically takes 2-8 minutes.
- Once thawed, gently mix bag to disperse clumps of cellular material and administer within 60 minutes. If more than 1 infusion bag is required on one day, only 1 bag should be thawed at one time and the next bag should not be thawed until infusion of the previous bag is complete.
- The 10 x 10⁶ dose of obe-cel (blue bag) is administered via a syringe as a slow push through a central venous line at approximately 0.5 mL/minute, while larger doses of 100 x 10⁶ (orange bag) and 300 x 10⁶ (red bag) are administered via intravenous bag infusion at 0.1 to 27 mL/minute.
- For syringe administration, the exact dose volume according to the Release for Infusion certificate is withdrawn from the blue bag with a syringe. Do not use a lymphodepleting filter or use the syringe to mix the cells.¹
- External resources for psychological, emotional, financial, lodging, transportation, community, education, nutrition and pet support are available on the AutolusAssist website.
- The manufacturer currently has a 24/7 case manager service, AutolusAssist.
- The case manager must be contacted to determine patient eligibility for the Patient Support Program that connects patients and caregivers to programs that can provide support for transportation, lodging, meals, and finances.¹²⁻¹³
References
1.Aucatzyl Prescribing Information. Autolus Inc, 2025. Accessed August 4, 2025. https://www.autolus.com/media/1sdfadp0/obe-cel-us-prescribing-information-and-medication-guide.pdf.
2.Roddie C, Sandhu KS, Tholouli E, et al. Obecabtagene Autoleucel in Adults with B-Cell Acute Lymphoblastic Leukemia. N Engl J Med. 2024;391(23):2219-2230. doi:10.1056/NEJMoa2406526
3.Roddie C, Tholouli E, Shaughnessy P, et al. Long-term efficacy and safety of Obecabtagene Autoleucel (OBE-CEL) in adult patients (PTS) with relapsed/refractory B-cell acute lymphoblastic leukemia ([R/R B-all]; pooled analysis from Allcar19 and Felix Phase IB studies) or other B-cell malignancies (allcar19 extension study). Blood. 2023;142(Supplement 1):2114-2114. doi:10.1182/blood-2023-180666
4.Roddie C, Dias J, O'Reilly MA, et al. Durable Responses and Low Toxicity After Fast Off-Rate CD19 Chimeric Antigen Receptor-T Therapy in Adults With Relapsed or Refractory B-Cell Acute Lymphoblastic Leukemia. J Clin Oncol. 2021;39(30):3352-3363. doi:10.1200/JCO.21.00917
5.Kymriah Prescribing Information. Novartis, 2025. Accessed August 4, 2025. https://www.novartis.com/us-en/sites/novartis_us/files/kymriah.pdf.
6.Tecartus Prescribing Information. Kite Pharma, 2025. Accessed August 4, 2025. https://www.gilead.com/-/media/files/pdfs/medicines/oncology/tecartus/tecartus-pi.pdf.
7.Hayden PJ, Roddie C, Bader P, et al. Management of adults and children receiving CAR T-cell therapy: 2021 best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE) and the European Haematology Association (EHA). Ann Oncol. 2022;33(3):259-275. doi:10.1016/j.annonc.2021.12.003
8.Hill JA, Seo SK. How I prevent infections in patients receiving CD19-targeted chimeric antigen receptor T cells for B-cell malignancies. Blood. 2020;136(8):925-935. doi:10.1182/blood.2019004000
9.Los-Arcos I, Iacoboni G, Aguilar-Guisado M, et al. Recommendations for screening, monitoring, prevention, and prophylaxis of infections in adult and pediatric patients receiving CAR T-cell therapy: a position paper. Infection. 2021;49(2):215-231. doi:10.1007/s15010-020-01521-5
10.Wat J, Barmettler S. Hypogammaglobulinemia After Chimeric Antigen Receptor (CAR) T-Cell Therapy: Characteristics, Management, and Future Directions. J Allergy Clin Immunol Pract. 2022;10(2):460-466. doi:10.1016/j.jaip.2021.10.037
11.Yáñez L, Alarcón A, Sánchez-Escamilla M, Perales MA. How I treat adverse effects of CAR-T cell therapy. ESMO Open. 2020;4(Suppl 4):e000746. doi:10.1136/esmoopen-2020-000746
12.Support & resources for patients & caregivers. Autolus Assist. Accessed May 12, 2025. https://www.autolusassist.com/patients-and-caregivers/.
13.Comprehensive support for providers & patients with AutolusAssist. Autolus. Accessed May 12, 2025. https://www.aucatzylhcp.com/support-resources/.