FDA grants accelerated approval to linvoseltamab-gcpt for relapsed or refractory multiple myeloma
What is the potential role for linvoseltamab-gcpt in the treatment of relapsed or refractory multiple myeloma?
- Linvoseltamab-gcpt (Lynozyfic) is a bispecific B-cell maturation antigen (BCMA)- direct CD3 T-cell engager.1 BCMA is expressed on plasmablasts and plasma cells.2 It has emerged as a useful drug target for the treatment of multiple myeloma.
- Lynozyfic is recommended for patients with relapsed/refractory multiple myeloma, after at least four prior lines of therapy including an anti-CD38 monoclonal antibody, a proteasome inhibitor (PI), and an immunomodulatory drug (IMiD).1
- Approval for the indication above was based on the LINKER-MM1 study.3
- The LINKER-MM1 trial was a phase 1/2, multicenter, open-label, multicohort trial assessing the safety and efficacy of Lynozyfic.
- Phase I enrolled patients were required to have double-class refractory multiple myeloma, specifically refractory to both an IMiD and PI.
- Phase II enrolled patients were required to have triple-class refractory multiple myeloma, specifically refractory to an IMiD, PI, and anti-CD38 antibody.
- Phase I
- The phase I dose escalation portion followed a modified 3 + 3 (4 + 3) dose-escalation design with a 28-day dose-limiting toxicity observation period.
- Phase II
- The primary objective of phase II was to assess the overall response rate.
- A full dose of linvoseltamab intravenous (IV) at either 50 mg or 200 mg was administered once a week from week 3 through week 14, after which patients transitioned to administration once every 2 weeks starting on week 16.
- Patients treated at a full dose of 200 mg transitioned to once every 4 weeks dosing if they achieved a very good partial response (VGPR) or better and had a minimum of 24 weeks on treatment.
- Treatment in phase II was continued until progressive disease (PD) or other discontinuation criteria were met.
- At a median follow-up of 14.3 months, the ORR was 71%, with 50% achieving complete response (CR) or better.
- In the 104 patients treated with 50 mg dosage level, with a median follow-up of 7.4 months, the ORR was 48%, with 21% achieving CR or better.
- The median duration of response (DOR) for 200 mg dosage level patients (n = 83) was 29.4 months (95% CI, 19.2 to not evaluable).
- Among 200 mg dosage level patients, the most common adverse events included cytokine release syndrome (35.0% Grade 1, 10.3% Grade 2, 0.9% Grade 3), neutropenia (0.9% Grade 2, 18.8% Grade 3, 23.1% Grade 4), and anemia (3.4% Grade 1, 4.3% Grade 2, 30.8% Grade 3).
- Immune effector cell-associated neurotoxicity syndrome occurred in 7.7% of patients (2.6% each Grade 1, Grade 2, and Grade 3). Infections were reported in 74.4% of patients (33.3% Grade 3, 2.6% Grade 4); infection frequency and severity declined over time.
- The LINKER-MM1 trial was a phase 1/2, multicenter, open-label, multicohort trial assessing the safety and efficacy of Lynozyfic.
- Other agents that are FDA approved for mulitple myeloma after at least four prior therapies include the following:
- CD3/BCMA Bispecific antibodies
- Elranatamab-bcmm5
- Teclistamab-cqyv6
- CD3/GPRC5D Bispecific antibody
- Talquetamab-tgvs7
- CD3/BCMA Bispecific antibodies
- Each of the recommended agents in this setting have a unique dose ramp-up schedule and route of administration. Previous therapies, target, ramp-up schedule, route, and side effect profile all play a role in which treatment is chosen for a patient.
- Linvoseltamab-gcpt dose ramp up schedule and route of administration is outlined in Table 1.
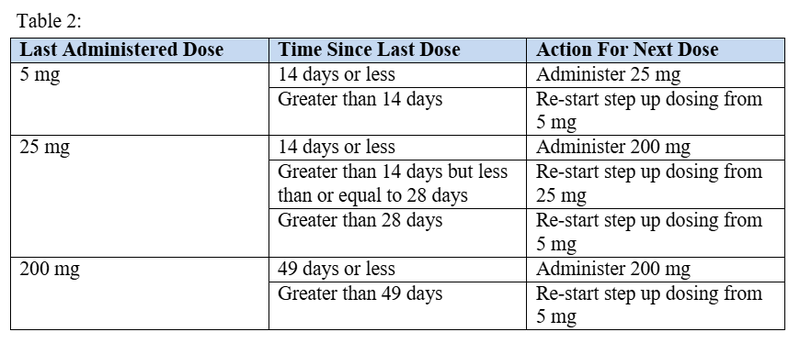
- Linvoseltamab-gcpt recommendations for re-starting therapy after a dose delay are outlined in Table 2.

What role can the pharmacist play in the management of patients on linvoseltamab-gcpt?
- Linvoseltamab-gcpt has a step-up dosing schedule consisting of a 5 mg dose on day 1 of treatment, a 25 mg dose on day 8 of treatment, and a 200 mg dose on day 15 of treatment.4
- Subsequent doses are 200 mg given once weekly from weeks 4 through 13 for a total of 10 treatment doses.
- Starting on week 14, dosing moves to a biweekly (every two weeks) schedule of 200 mg given every two weeks for the duration of therapy.
- Every 4-week dosing can be considered for patients who have achieved and maintained VGPR or better at or after week 24 of treatment and have received at least seventeen 200 mg doses.
- Infection prevention is another area in which pharmacists play a large role
- Consensus recommendations state bacterial, viral, and PJP prophylaxis are necessary in patients with multiple myeloma receiving BITE therapy.8
- Bacterial prophylaxis with broad spectrum antimicrobials is recommended during periods of neutropenia, viral prophylaxis is recommended throughout therapy, and PJP prophylaxis is also recommended throughout therapy.8
- Pharmacists can educate caregivers on signs/symptoms of cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) and assist providers in their management.
- The incidence of CRS among patients in the LINKER-MM1 trial was 46% and the incidence of ICANS was 8%.3
- If patients develop symptoms of CRS or ICANS between grades 1 and 3, Lynozyfic should be withheld, and supportive care should provided as directed by the CRS/ICANS management recommendations.9
- For grade 4 CRS or ICANS, Lynozyfic should be permanently discontinued.4
- Infusion-related reactions occurred in approximately 9% of patients receiving linvoseltamab-gcpt. Grade 2 and 3 infusion reactions warrant supportive care and a decreased infusion rate, while grade 4 infusion reactions warrant a permanent discontinuation of linvoseltamab-gcpt.4
- Pharmacists can play a role in the selection of pre-medications for Lynozyfic for both primary and secondary infusion reaction prophylaxis.
- Pre-medications include acetaminophen 650-1000 mg orally 30-60 minutes prior to the infusion; diphenhydramine 25 mg intravenously or orally 30-60 minutes prior to the infusion; and dexamethasone (or equivalent) 1-3 hours prior to the infusion dosed at 40 mg before the first and second step up dose, and first treatment dose.4
- Subsequent doses of dexamethasone, if patients tolerate the infusion without CRS, can be dosed at 10 mg given 1-3 hours prior to the infusion.4
- Recommendations for slowed infusion rates can also be made.
- Pharmacists can play a role in the selection of pre-medications for Lynozyfic for both primary and secondary infusion reaction prophylaxis.
- Grade 4 infections and non-hematologic adverse reactions warrant the consideration of permanent discontinuation of linvoseltamab-gcpt.4
- Pharmacists can also play a role in dose recommendations secondary to fluctuations in platelet count, hemoglobin, and ANC.4
- To date, no specific drug interactions have been published by the manufacturer or cited in the compendia. Despite this, a general recommendation may be to use caution when prescribing linvoseltamab-gcpt in combination with CYP450 substrates within the first 14 days after the first 200 mg treatment dose.4
- Pharmacists also play a role in formulary management.
- As there are multiple approved bispecific agents for multiple myeloma, pharmacists can help determine which agents to keep, remove, or add to an institutional formulary.
- Pharmacists can assess the utilization within their patient population as well as the cost to both patients and health systems.
- Linvoseltamab-gcpt has an associated REMS program which can also be managed by pharmacy staff to ensure safe use for each patient.
Clinical Pearls
- Linvoseltamab-gcpt is available as single dose vials in the following strengths4
- 5mg/2.5 mL (2 mg/mL)
- 200mg/10mL (20 mg/mL)
- Linvoseltamab-gcpt must be diluted in a 0.9% Sodium Chloride injection prior to administration. The diluted solution remains stable at room temperature for no more than 8 hours but remains stable under refrigeration (2-8ºC) for no more than 48 hours.4
- The use of a 0.2-5-micron filter is required.
- Tubing must be primed with Lynozyfic.
- Linvoseltamab-gcpt infusions must be administered by a healthcare professional with immediate access to emergency equipment and support to manage severe reactions.4
- Patients should be hospitalized for ~24 hours after administration of the first step-up dose, and for ~24 hours after the second step-up dose.4
- Regeneron provides the Lynozyfic Surround program which helps eligible patients access linvoseltamab-gcpt and navigate their health insurance authorization process. There is both a commercial copay program and patient assistance program offered that can be accessed via the Lynozyfic website.10
References
1.Lynozyfic (linvoseltamab-gcpt) Receives FDA Accelerated Approval for Treatment of Relapsed or Refracoty Multiple Myeloma. Food and Drug Administration. Accessed September 30, 2025. https://investor.regeneron.com/news-releases/news-release-details/lynozyfictm-linvoseltamab-gcpt-receives-fda-accelerated-approval.
2.Tai YT, Anderson KC. Targeting B-cell maturation antigen in multiple myeloma. Immunotherapy. 2015;7(11):1187-99. doi: 10.2217/imt.15.77.
3.Bumma N, Richter J, Jagannath S, et al. Linvoseltamab for treatment of relapsed/refractory multiple myeloma. Journal of Clinical Oncology. 2024;42(22):2702-2712. Doi:10.1200/JCO.24.01008.
4.Lynozyfic-gcpt. Package insert. Regeneron; 2025.
5.Elranatamab-bcmm. Package insert. Pfizer. 2025.
6.Teclistamab-cqyv. Packager insert. Johnson & Johnson. 2025.
7.Talquetamab-tgvs. Package insert. Johnson & Johnson. 2025.
8.Raje N, Anderson K, Einsele H, et al. Monitoring, prophylaxis, and treatment of infections in patients with MM receiving bispecific antibody therapy: consensus recommendations from an expert panel. Blood Cancer J. 2023;13(1):116. doi:10.1038/s41408-023-00879-7
9.Ludwig H, Terpos E, van de Donk N, et al. Prevention and management of adverse events during treatment with bispecific antibodies and CAR T cells in multiple myeloma: a consensus report of the European Myeloma Network. Lancet Oncol. 2023;24(6):e255-e269. doi:10.1016/S1470-2045(23)00159-6
10.Lynozyfic Surround. Lynozyfic HCP. Accessed September 30, 2025. https://www.lynozyfichcp.com/support-resources/LYNOZYFIC-surround