FDA grants accelerated approval to dordaviprone for diffuse midline glioma
What is the potential role of dordaviprone in the treatment of recurrent H3 K27M-mutant diffuse midline glioma?
- Diffuse midline gliomas (DMGs) are aggressive brain tumors that develop in central structures such as the thalamus, brainstem, and spinal cord. 1
- They primarily affect children aged 3 to 10 but can also occur in young adults.
- DMGs are the second most common malignant brain tumor in children, with an estimated 200–300 cases annually in the U.S. 2
- Depending on the tumor’s location and grade, patients may present with a wide range of symptoms of varying severity, most commonly progressive neurological deficits such as persistent headaches, dizziness, ataxia, unilateral weakness or paralysis, speech impairment, vision or hearing changes, and seizures.1
- Behavioral changes, including emotional or personality alterations, may also occur when critical brain regions are affected.1
- DMG typically have a poor prognosis due to the infiltrative nature of the tumor and their intrinsic resistance to therapies, which together make complete surgical removal challenging and reduce the effectiveness of pharmacological therapies.1
- The hallmark genetic alteration in DMGs is a point mutation in the histone H3 gene, where lysine (K) is replaced by methionine (M) at position 27 (H3K27M).
- This mutation occurs in up to 80% of pediatric cases and about 60% of adult cases, and is associated with poorer overall survival and reduced response to therapy compared to H3 wild-type tumors. 3
- The first line and only established therapy for patients with H3 K27M disease is radiation, which has been shown to modestly improve the survival rate, with a mean overall survival of 12.0 months and a high recurrence rate.4
- Dordaviprone is the only FDA-approved systemic therapy for recurrent H3 K27M-mutant diffuse midline glioma in both pediatric patients and adults.5
- It has two potential mechanisms of action: antagonizing dopamine receptor D2/3 and activating mitochondrial caseinolytic protease P (ClpP). Hyperactivation of ClpP leads to degradation of mitochondrial proteins with subsequent energy depletion and apoptosis of H3 K27M-mutant glioma cells.6
- Approval for this indication was based on an integrated efficacy analysis from 5 open-label, non-randomized studies, including three clinical trials: ONC006 (phase 1), ONC013 (phase 2), ONC014 (phase 2), one single-patient compassionate use program: ONC016, and an expanded access program: ONC18
- Methods:
- Includes 46 adults and 4 pediatric patients with recurrent and/or progressive H3K27M-mutant diffuse midline glioma.6
- Eligible patients were required to have measurable disease per the Response Assessment in Neuro-Oncology (RANO) criteria for high-grade gliomas (HGG), were 2 years and older, had a Karnofsky/Lansky performance score of ≥ 60, received prior radiation therapy with a washout of at least 90 days before the first dordaviprone dose and sufficient washout for other systemic therapies including 23 days for temozolomide, 42 days for bevacizumab and 28 days for other antitumor agents.7
- Dosing: adult patients received 625 mg orally (125 mg per capsule), whereas pediatric doses were allometrically scaled by body weight using a ¾ power model (based on 70 kg adult weight) and rounded to the nearest capsule size. The frequency of once weekly or every 3 weeks, depending on the study design. 6
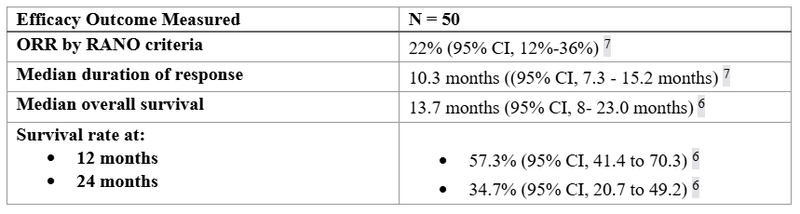
- The primary endpoint was the overall response rate (ORR) per RANO-HGG criteria, including complete and partial responses. Complete response is defined as the disappearance of all enhancing diseases for more than 4 weeks with no new lesions, while partial response requires at least a 50% reduction in enhancing lesion size for more than 4 weeks without new lesions or clinical worsening. 7
- Results:
- Methods:
- Safety was evaluated in 376 patients from 4 open-label studies:
- Most common adverse events (>20%) include fatigue (34%), headache (34%), nausea (24%), vomiting (24%), and musculoskeletal pain (20%). Most rated as grade 1 or 2.7
- The most common (≥2%) Grade 3 or 4 laboratory abnormalities are decreased lymphocytes (7%), decreased calcium (2.7%), and increased alanine aminotransferase (2.4%).7
What role can the pharmacist play in the management of patients on dordaviprone?
- Pharmacists can play a role in dordaviprone management, including medication dosing, drug-drug interactions, and toxicity
- Dosing:
- Dordaviprone comes as a 125 mg capsule and has a different dosing regimen for adults and the pediatric population
- Adult: 625 mg once weekly
- Pediatric: 125-625 mg dosed by body weight once weekly.
- Dordaviprone comes as a 125 mg capsule and has a different dosing regimen for adults and the pediatric population
- Dosing:
- Recommended dosage for pediatric patients based on body weight:
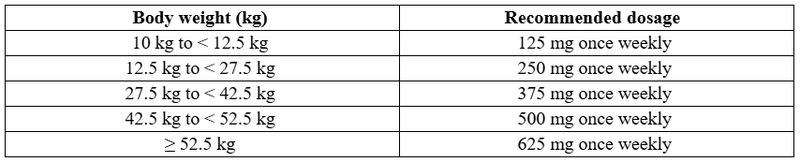
- Dose reduction can be considered for adverse reactions

- There is no dosing adjustment for renal/hepatic impairment studied in approved trials.7
- Drug-drug interactions:
- 3A4 modifiers: dordaviprone is a CYP3A4 substrate. Avoid concomitant use of strong and moderate CYP3A4 inhibitors or inducers with dordaviprone. Reduce the dose per manufacturer recommendations if CYP3A4 inhibitors cannot be avoided.7
- QTc-prolonging medications: dordaviprone can prolong the QTc interval. Avoid using concurrently with products known to prolong the QTc interval, or separate administration and increase the frequency of QTc monitoring if impossible to avoid.7
- Notable toxicity management:
- QTc prolongation (12% of 82 patients experienced QTc prolongation)
- Monitor ECGs and electrolytes prior to starting dordaviprone and periodically as indicated.
- If QTc absolute value > 500 ms or an increase of 60 ms from baseline: interrupt dordaviprone until QTc interval ≤ 480 ms or return to baseline before resuming at the next lower dose level.
- In serious life-threatening arrhythmia (torsades de pointes, polymorphic ventricular tachycardia), discontinue permanently.
- Hypersensitivity (0.3% of patients had severe sensitivity). Can consider interrupting and initiating supportive care or discontinuing in severe reactions.
- Embryo-Fetal Toxicity:
- Dordaviprone can cause fetal harm. Confirming pregnancy status prior to starting the medication.
- Advise females of reproductive potential or males with partners of reproductive potential to utilize effective contraception during therapy and for 1 month after the last dose.
- QTc prolongation (12% of 82 patients experienced QTc prolongation)
- Patient assistance program through ChimerixCares:
- Support is available to assist with insurance navigation, prior authorization, claims, and medication access for uninsured or underinsured patients.
- Temporary free supply is available to start or continue treatment while waiting for prior authorization approval.
Clinical Pearls
- Capsules must be swallowed whole and should not be crushed, chewed, or dissolved. For patients unable to swallow capsules, the contents may be mixed with 15–30 mL of liquid and administered within 2 hours.
- Capsules are taken on an empty stomach, at least 1 hour before or 3 hours after meals.
- If a dose is missed, it should be taken as soon as possible unless the next dose is due within 12 hours. Two doses should not be taken on the same day.
- If vomiting occurs after a dose is taken, an additional dose should not be taken, and the next dose should be taken at its scheduled time.
- Dordaviprone is currently the only FDA-approved systemic treatment for recurrent H3K27M-mutant diffuse midline glioma in both adults and pediatric patients through five open-label, non-randomized clinical trials conducted in the U.S. (ONC006 [NCT02525692], ONC013 [NCT03295396], ONC014 [NCT03416530], ONC016 [NCT05392374], and ONC018 [NCT03134131])
- It is important to note that clinical trials exclude patients with diffuse intrinsic pontine glioma (DIPG), primary spinal tumors, or leptomeningeal disease. Only patients with H3 K27M mutations with measurable progressive disease post-radiation therapy were included.
- Notably, the ACTION trial (NCT05580562) is an ongoing international, randomized, double-blind, placebo-controlled, phase 3 study evaluating dordaviprone in newly diagnosed H3 K27M-mutant diffuse glioma patients who have completed standard radiotherapy.
References
1.Al Sharie S, Abu Laban D, Al-Hussaini M. Decoding Diffuse Midline Gliomas: A Comprehensive Review of Pathogenesis, Diagnosis and Treatment. Cancers. 2023;15(19):4869. doi:10.3390/cancers15194869
2.Tosi U, Souweidane M. Diffuse Midline Gliomas: Challenges and New Strategies in a Changing Clinical Landscape. Cancers. 2024;16(1):219. doi:10.3390/cancers16010219
3.Saratsis AM, Knowles T, Petrovic A, Nazarian J. H3K27M mutant glioma: Disease definition and biological underpinnings. Neuro-Oncol. 2023;26(Suppl 2):S92-S100. doi:10.1093/neuonc/noad164
4.Gallitto M, Lazarev S, Wasserman I, et al. Role of Radiation Therapy in the Management of Diffuse Intrinsic Pontine Glioma: A Systematic Review. Adv Radiat Oncol. 2019;4(3):520-531. doi:10.1016/j.adro.2019.03.009
5.Nabors LB, Horbinski C, Pinho MC. NCCN Guidelines Index Table of Contents Discussion. Published online 2025.
6.Arrillaga-Romany I, Gardner SL, Odia Y, et al. ONC201 (Dordaviprone) in Recurrent H3 K27M–Mutant Diffuse Midline Glioma. J Clin Oncol. 2024;42(13):1542-1552. doi:10.1200/JCO.23.01134
7.Wen PY, Macdonald DR, Reardon DA, et al. Updated Response Assessment Criteria for High-Grade Gliomas: Response Assessment in Neuro-Oncology Working Group. J Clin Oncol. Published online April 10, 2010. doi:10.1200/JCO.2009.26.3541
8.modeyso.en.USPI.pdf. Accessed October 30, 2025. https://pp.jazzpharma.com/pi/modeyso.en.USPI.pdf